There’s a lot that needs to be taken into consideration when assessing a new client.
Their unique injury history (past and present), goal(s), training experience, time constraints, equipment availability, even their favorite 90’s tv teen drama (if it’s not Party of Five we can’t be friends)…
…all are taken into account and cross-pollinated with my educational background and experience to ascertain, to the best of my ability, what will be the best course of action to get said individual from Point A1to Point B2 this means becoming in the most time efficient and and safe manner possible.
The assessment, at least from my perspective, is an amalgamation of muscle testing, movement screens, table work, and good ol’ fashioned investigative work to see whether or not something shakes free or if any “red flags” exist.
But more importantly, the assessment is a splendid opportunity to set the tone, prove to someone that they’re not “broken,” and to help them find their TRAINABLE MENU.
In short, I often joke that my assessment can be described as follows:
“Can the person standing in front of me do stuff?”
There’s only so much muscle testing, table work, looking at range of motion, and “hmmm’ing” and “ahhhh’ing” any one individual can tolerate before (s)he wants to jump through a pane glass window.
To that end, I prefer to make my assessments more palatable by getting the person standing/sitting in front of me more involved in the process and providing the “facade” (for lack of a better term) that they’re being taken through a pseudo training session.
By having him or her MOVE during their assessment I accomplish a few things:
1) I don’t come across as a creepoid by just staring at them for 60 minutes and stroking my beard (even though I don’t have one).
2) I get waaaaaaay more information in terms of movement ability, compensation patterns (if any) that exist, and whether or not certain positions (or loads) exacerbate their symptoms.
Active vs. Passive Assessment
One simple way to do all the above is to differentiate between one’s ability to actively perform a specific movement pattern and to passively do it.
My colleague, Luke Worthington, who’s my co-presenter in the Strategic Strength Workshop, states things very succinctly:
“What can THEY do?” = Active Assessment
“What can I do FOR them?” = Passive assessment.
Lets take the squat as an example.
When you watch someone perform a standard bodyweight (or loaded) squat you’re bound to see a bevy of things go awry.
Don’t get me wrong, it’s not always a shit show.
Every so often I’ll work with someone for the first time, they’ll demonstrate a well executed squat, and I’ll break down crying like the first time I watched the series finale of Andor.
However, if I’m being honest, this doesn’t happen often.3
Generally speaking there’s always something weird or wonky or twingey whenever I watch someone squat
No one is perfect.
But to that point, I think it’s imperative to differentiate between someone’s ACTIVE ability to do something and their PASSIVE ability to do it.
Watch someone squat and it’s likely you’ll see any one of the following (if not a combination):
Knee valgus
Excessive rounding of the spine
Excessive pronation of the feet
Loss of balance
A perceived lack of depth (<— which is arbitrary, but if there’s a lot of “effort” to get to a certain depth or it’s just really, really shallow, then that is important to note).
And when we do see any of the above we have a nasty habit of assuming that said individual is dysfunctional, and subsequently end up over corrective exercising them to death.
Fast forward three months (and a cornucopia of hip mobility and ankle dorsiflexion drills) and there’s been little, if any, improvement.
But don’t stop there; especially if you find they’re having trouble with it.
You should also test them PASSIVELY.
Oftentimes, when you add this extra layer of assessment, in a way that’s less aggressive and provides a bit more stability to the system – FYI: HERE‘s another way to do it in a quadruped position – you’ll find that they CAN do what you’re asking them to do.
Why Is This Important?
In the video above I’m taking my training partner, Justin, through a basic (passive) hip scour/hip flexion screen. If he were a client this would follow an active squat assessment.
I’d want to see if his ACTIVE movement (he’s doing the work) matched his PASSIVE (I’m doing the work). From there I’d want to compare the gap that exists between the two.
I want that gap to be as narrow as possible.
If his active squat was poor yet I re-assessed passively and saw an improvement – I.e., that he could, indeed, access more ROM – then I can surmise with a high degree of certainty that he doesn’t have a micro-penis he is likely not dealing with something more nefarious, like a bony block or musculature issue.
In this scenario I can do my job as a coach.
I can implement the appropriate “correctives” and/or exercise progressions/regressions to help him learn to squat.
His body showed me he can do it passively, so I need to show it how to do it actively.
If, however, there was no improvement when testing him passively, then:
It’s not my job.
1) I’d still work within my scope and train him within the ROM that’s pain free and that he can control.
2) However, I’d also refer out for more diagnostic testing or manual therapy to compliment his iron work.
Take Home Points
The assessment shouldn’t be used as a tool to point out every…single…dysfunction someone has.
Besides, what presents as “dysfunctional” actively may just be the body turning on the emergency brakes.
Also look at PASSIVE movement.
Try to narrow the gap between active ROM and passive.
If more ROM is present passively, then do what you do best…coach!
If ROM is poor (or pain exists) actively AND passively, you may want to consider referring out.
I don’t know, it could just be me, but Groutfits make my butt look amazing.
I often speak on the importance of the test/re-test concept with regards to assessment.
It’s nothing fancy or elaborate.
You test something – whether it be range of motion or maybe a strength discrepancy – implement a “corrective” modality if something’s deemed out of whack, and then re-rest that shit to see if it worked.
The test/re-test approach helps set the tone for any future “corrective” strategies or programming considerations you’ll do as a coach or trainer.
In addition, and something I’d argue is equally as important, it also provides an added layer of value to the assessment.
If you’re able to demonstrate to someone a significant change or improvement in ROM or reduction in pain/discomfort by implementing a drill or two, and it’s something they’ve been struggling with despite countless interactions with other fitness professionals, what’s the likelihood they’ll bust out their checkbook or Bitcoin wallets (<—depending on their level of geekery)?
I suspect highly likely.
It demonstrates a perceived level of “mastery” and knowledge-base towards the assesser (you) and, in a roundabout, reverse psychology kind-of-way, delves into the “pain center” of the assessee (athlete/client).
In this example it can refer to literal pain such as a banged up shoulder, knee, or lower back. But it can also speak to pain in the figurative sense too. Someone who’s frustrated and “had it up to here!” that they can’t lose weight, or maybe an athlete who was cut from their high-school team would have a degree of “pain” that would incentivize them to take action.
Show someone success or a clear path of action, however little, and they’re putty in your hands.
Of course this assumes you’re not some shady shyster who tries to up-sell the benefits of some super-secret concurrent, 47-week, Eastern-Bloc training program you copied from Muscle & Fitness or, I don’t know, organic raspberry ketones laced with mermaid placenta.
People who promote and use smoke-and-mirror tactics are the worst.
But lets get back to the topic at hand.
Test/Re-Test
One of the main screens I use with my athletes and clients is their ability to lift or elevate their arms above their heads.
Shoulder flexion is important for everyone, not just overhead athletes and CrossFitters.
If someone lacks shoulder flexion, and they’re an athlete, it’s going to affect their performance. A baseball pitcher may be “stuck” in gross shoulder depression, which in turn will have ramifications on scapular positioning and kinematics, which in turn will result in faulty mechanics and compensatory issues up and down the kinetic chain.
Conversely, regular ol’ Hank from accounting, who likes to hit the gym hard after work, if he lacks shoulder flexion, he too could have numerous issues arise ranging from shoulder and elbow pain to lower back shenanigans.
Shoulder flexion – and the ability to do it – is a big deal in my opinion. And it’s a screen that should be a high-priority in any fitness professionals assessment protocol.
So lets say I’m working with someone who lacks shoulder flexion. I test it both actively (standing, picture above) and passively (on a training table).
I surmise that it’s limited and that it may be feeding into why a particular person’s shoulder has been bothering him or her.
I can use the test/re-test approach to see if I can nudge an improvement.
Now, as I’ve learned from many people much smarter than myself – Mike Reinold, Sue Falsone, Dr. Evan Osar, Dr. Stuart McGill, Papa Smurf, etc – you shouldn’t rely on any ONE screen/corrective.
Everyone is different, and what works for one person might not even scratch the surface for another.
With regards to addressing (lack of) shoulder flexion5, there are a handful of “go to” strategies I like to use.
And then it’s just a matter of seeing which one sticks.
1) Encouraging a Better Position
In order to elevate the humerus (arm) above your head, the scapulae (shoulder blade) needs to do three things:
Upwardly rotate
Posteriorly tilt
Protract
The ability to do so is vastly correlated with the thorax. Those who are super kyphotic (ultra rounded upper back) will have a hard time elevating their arms overhead. Often, the simple “fix” here is to foam roll the upper back and work on more t-spine extension and you’ll almost always see an improvement.
Bench T-Spine Extension
Side Lying Windmill
But what about the opposite? Those who are stuck in more “gross” extension and downward rotation?
I.e., the bulk of athletes and meatheads.
Here the shoulder blades can be seemingly “glued” down.
In that case some positional breathing drills to “un-glue” the shoulder blades (and to encourage more 3D or 360 degree expansion of the ribcage/thorax) would be highly advantageous.
All 4s Belly-Breathing
It’s amazing what a few minutes of this drill can do with improving shoulder flexion ROM, without having to yank or pull or “smash” anything.
2) Allow the Shoulder Blades to Move
Some people simply don’t know how to allow their shoulder blades to move. A prime example is this past weekend.
An attendee who’s a personal trainer – but also competes in figure – mentioned how her shoulders (especially her left) had been bothering her for eons, and she couldn’t figure out why.
We had her perform this drill.
1-Arm Quadruped Protraction
In reality, both protraction and retraction are occurring, but many people have a hard time with the former.
The idea here is to learn to gain movement from the shoulder blade itself and not via the t-spine.
Here’s another angle (because, triceps):
https://www.youtube.com/watch?v=eyNFNxqFlSc
After a few “passes” with this drill, she saw an immediate improvement in her ROM. What’s more, the following day when she showed up for Day #2, the first thing out of her mouth was “my shoulder feels amazing today.”
That’s a win.
3) Pin and Go
Another route to take is to have the person foam roll their lats. Not many people do this, and there’s a reason why: It’s un-pleasant.
I’ll have the person spend a good 30 seconds or so on each side and then have them stand up and perform a simple SMR drill using a lacrosse ball against a wall.
They’ll “pin” the teres minor down (basically, find the tender spot behind their shoulder and hold it there) and then work into upward rotation.
https://www.youtube.com/watch?v=9OiGt_O1FvY
Another five or so passes here, and I’ll re-test.
Many times I’ll see a marked improvement in their shoulder flexion.
Caveat
NONE of this is to insinuate that anything mentioned above will work for everyone. The idea is to understand that it’s important to “test” a number of modalities and then re-test to see if you find an improvement.
If you do, you’re likely barking up the right tree which will make your corrective approach and subsequent strength training more successful.
I remember when Julian was first born my wife and I had many, many “checklists” to make sure that our schedules were in line so that we knew who was doing what, and when to make sure that 1) Julian would be fed and 2) he’d get his naps in. We weren’t playing games with that shit.
It’s funny, though. It’s been a trip to see how I make connections and correlations between that and stuff I see and come across in my professional life… training and coaching athletes/clients.
One of the purest examples is something I witness on an almost weekly basis.
Many of the new people who start with me are beginner or intermediate level meatheads (male and female) who, for whatever reason(s), have been dealing with a pissed off shoulder that inhibits their ability to train at the level or intensity they’d like. It’s frustrating on their end and it’s my job as the coach to try to peel back the onion and see what may or may not be the root cause or causes.
That being said, I try not to go too deep down the rabbit hole. There’s a fine line between doing your due diligence as their coach and figuring out what may be causing their shoulder ouchies and making them feel like a patient.
READ: No one, and I mean NO ONE likes go to their personal training session and do rehab exercises for an hour. I’d surmise most would rather jump into a pool of lava. To that end, here’s my quick “go to checklist” whenever I have a client express that their shoulder hates them at the moment.
The “My Shoulder Hurts” Checklist
1) Technique
Most commonly people will note how bench pressing bothers their shoulder(s). Working on their technique is the baby check list equivalent of blow out explosive diarrhea.
I.e., It’s code mother-fucking red.
Following the mantra “if it causes pain, stop doing it” is never a bad call, and I am all for nixing any exercise or drill that does such a thing. However, I don’t like to jump to conclusions too too quickly. Sometimes making a few minor adjustments to someone’s technique or setup can make all the difference in the world.
Almost always I’ll have to spend some time on their set-up. I like to cue people to start in a bridge position to drive their upper traps into the bench and to set their scapulae (together AND down).
We can make arguments as to what this is actually doing. Some will gravitate towards it improving joint centration. Cool (and not wrong). I like to keep a little simpler and note that all it really does is improve stability.
A post shared by Tony Gentilcore (@tonygentilcore) on
Another thing to note is many people tend to flare their elbows out too much when they bench which leaves the shoulders out to dry and in a vulnerable position.
MINOR NOTE: Since recording that video above (many years ago), I have since changed my views slightly thanks to some cueing from Cressey Sports Performance coach Tony Bonvechio. Elbows tucked on the way down is still something I’m after (albeit some are too aggressive at the expense of placing too much valgus stress on the elbows). However, when initiating the press motion, in concert with leg drive, allowing the elbows to flare out a teeny tiny bit (in an effort to keep the joints stacked and to place the triceps in a more mechanical advantage) will often play huge dividends in performance.
In the end, much of the time it comes down to people not paying any attention to how crucial their set-up is. It’s amazing how often shoulder pain dissipates or disappears altogether with just a few minor adjustments.
2) What People Don’t Want to Hear: Stop Benching, Bro
This is where the Apocalypse begins. Telling a guy (usually not women, they could care less) that he should probably stop benching for the foreseeable future is analogous to telling a CrossFittter they can’t tell you they CrossFit.
The thing about holding a barbell is that it “locks” the glenohumeral joint into internal rotation which can be problematic for a lot of people and often feeds into impingement syndrome.
[The rotator cuff muscles become “impinged” due to a narrowing of the acromion space.]
NOTE: I hate the term “shoulder impingement” because it doesn’t really tell you anything. There are any number of reasons why someone may be impinged. Not to mention there are vast differences between External Impingement and Internal Impingement….which you can read about in more detail HERE.
If bench pressing hurts, and we’ve tried to address technique, I’ll often tell them to OMIT barbell pressing in lieu of using dumbbells instead. With DBs we can utilize a neutral grip, externally rotate the shoulders a bit more, and open up the acromion space.
Or, maybe they can still barbell press, albeit at a decline. When you place the torso at a decline the arms can’t go into as much shoulder flexion and you’re then able to avoid the “danger zone.”
If all else fails, sadly, you may have to be the bearer of bad news and tell someone that (s)he needs to stop benching for a few weeks to allow things to settle down.
3) Let the Scaps Move, Yo
Above I mentioned the importance to bringing the shoulder blades together and down in an effort to improve stability.
If you want to lift heavy shit, you need to learn to appreciate the importance of getting and maintaining tension. That said, if lifting heavy shit hurts your shit, we may need to take the opposite approach. Meaning: maybe we just need to get your shoulder blades moving.
When the scaps are “glued” together and unable to go through their normal ROM it can have ramifications with shoulder health. Push-ups are a wonderful anecdote here.
Unlike the bench press – an open-chain exercise – the push-up is a closed-chain exercise (hands don’t move) which lends itself to several advantages – namely scapular movement.
4) More Rows
This one will be short and sweet. Perform more rows. Many trainees tend to be very anterior dominant and spend an inordinate amount of time training their “mirror muscles” at the expense of ignoring their backside. This can lead to muscular imbalances and postural issues.
This makes me sad. And, when it happens, a kitten becomes homeless.
You sick bastard.
The easy fix is to follow this simple rule: For every pressing motion you put into your program, perform 2-3 ROWING movements. Any row, I don’t care.6
5) Address Scapular Positioning
I’m going to toss out an arbitrary number and I have no research to back this up, but 99% of the time when someone comes in complaining of rotator cuff or shoulder issues the culprit is usually faulty scapular mechanics. Sometimes people DO need a little more TLC and we may need to go down the “corrective exercise” rabbit hole.
The scapulae perform many tasks:
Upwardly and downwardly rotate
Externally and internally rotate
Anteriorly and posteriorly tilt.
AB and ADDuct (retract and protract).
Will clean and fold your laundry too!
They do a lot. And for a plethora of reasons, if they’re not moving optimally it can cause a shoulder ouchie. Sometimes people are too “shruggy” (upper trap dominant) with overhead movements, or maybe they’re stuck in downward rotation? Maybe they can’t protract enough and need more serratus work? Maybe they lack eccentric control and need a heavy dose of low trap correctives?
It dumbfounds me the number of times I have had people come in to see me explaining how they had been to this person and that person and NO ONE took the time to look at how their shoulder blades move.
I don’t like to get too corrective too soon, but if I’ve exhausted all of the above and stuff still hurts….it’s time to dig deeper.
If only there were a resource that dives into this topic in a more thorough fashion.
A few weekends ago I was in London teaching a workshop with my friend Luke Worthington.
We had a group of 35 trainers from across the UK (and Europe) eager to learn more about assessment, program design, coaching up common strength movements, and how I rank the Bourne movies.7
One of the main umbrella themes we kept hammering home was that, contrary to popular belief, “tight” hamstrings isn’t really a thing.
Labelling the hamstrings as “tight” is often the default scapegoat and blamed for everything from butt wink to low back pain to male pattern baldness. So it wasn’t surprising to see the flabbergasted reactions from the majority of attendees when Luke and I kept repeating our message.
You would have thought Gandalf rode in on a Unicorn yelling “You shall not stretch the hamstrings!” based on people’s facial expressions.
What’s next: Water isn’t wet? Grass isn’t green? Ryan Gosling’s gaze doesn’t penetrate my soul?
Listen, I’m as skeptical as they come whenever anyone in the health/fitness industry uses the words “everyone,” “always,” or “never.”
Those are three words, when used ad nauseam, immediately scream “shady motherfucker with an agenda,” whenever I hear them.
It’s never the hamstrings. OR You should never eat past 7 pm.
Always avoid gluten. OR If you’re serious about fat loss, always avoid carbs.
Everyone must deadlift from the floor. OREveryone who reads this site is clearly off the charts intelligent and attractive. (<— 100% true).
There are nevertheless exceptions to every rule and circumstance. I’d be remiss not to tip my hat at the notion there are, indeed, people out there who have legitimately tight (or, more to the point, anatomically short) hamstrings.
That being said, I doubt you’re one of them.
I’m not going to sit here and say it’s never the case, but it’s such a rare occurrence that you’re more likely to win an arm wrestling match vs. a grizzly bear than actually having tight/short hamstrings.
Take butt wink for example.
The common culprit is tight hamstrings (photo on the right).
But if we were to discuss (and respect) basic anatomy we’d note the following:
My pecs can cut diamonds.
The hamstrings are a bi-articular muscle group that cross both the hip and knee joints.
As we descend into deep(er) hip flexion – I.e., squat – the hamstrings lengthen on one end (hips) and shorten on the other (knee), for a net change of nada.
#itsnotthehamstrings.
But How Can We Tell?
It’s uncanny how many people I’ve interacted with in my career who describe having tight hamstrings, and after telling me they’ve been stretching them for 43 years (<— only a slight exaggeration), are still looking for that one magical stretch to cure them.
My first step is to plop him or her on an assessment table and ask them to perform a simple screen to ascertain whether or not they do, in fact, have tight hamstrings.
You lie the individual supine and ask them to slowly, while keeping one leg cemented to the table or floor, elevate the other off the table while keeping it as straight as possible. They keep going until they feel the first smidgeon of resistance (or you start to see compensations like the pelvis rotating, the foot rotating, and/or either knee start to flex).
An acceptable ROM is anywhere from 70-90 degrees of hip flexion.
A funny thing almost always happens.
Most people pass the screen with flying colors.
Me:“You don’t have tight hamstrings.”
Them: “The fuck outta here! You mean, there aren’t any other stretches I should be doing?”
Me:“Zero.”
Them: “Zero?”
Me:“Yep, zero.”
[Cue crickets chirping]
This finding doesn’t, however, dismiss the fact said person’s hamstrings still FEEL tight.
So, W……..T……….F?
Something is awry.
To peel back the onion a bit more I’ll then implement a brilliant trick I was reminded of by Ottawa based personal trainer, Elsbeth Vaino.
The Bridge Test
I’ll have the same individual perform a standard glute or hip bridge. They’ll get into position and then I’ll ask “where do you feel that?”
Many will immediately say “hamstrings.”
I’ll then have them perform a 1-Leg Glute Bridge and ask them to hold that position for 10-15 seconds.
Most don’t last five.
“YOWSA…..my hamstrings cramped up.”
Why?
The body’s #1 hip extensor is the glute max, and if it’s not doing it’s job well the body’s #2 hip extensor, the hamstrings, will pick up the slack.
In all likelihood, for most people most of the time, the hamstrings feel tight because 1) they’re overactive and doing double the work and/or 2) pelvic alignment needs to be addressed (more glutes and anterior core = more posterior pelvic tilt = hamstrings are put on slack).
NOTE: the latter point – hamstrings lengthened due to (excessive) anterior pelvic tilt – is why stretching them only feeds the issue. The tightness many feel is neural in nature, not because of true shortness. Stretching an already lengthened muscle only exacerbates things.
Something Else to Consider: Active End-Range Hip Flexion
To add another nail into the “it’s not the hamstrings” coffin I’ll also take a gander at one’s ability to move their hip into (active) end-range flexion.
This “trick” digs into some of Dr. Andreo Spina‘s work on Functional Range Conditioning (FRC) and is another splendid way to gently tell someone to stop stretching their hamstrings.
No diggidy, no doubt.
Final Word
The sensation of tight hamstrings is less about an anatomically short muscle which requires endless hours of static stretching, and more about improving:
Position/alignment of the pelvis via nudging people into a little more posterior pelvic tilt by hammering glutes and anterior core.
Active end-range hip flexion. Allow people to experience this position more often and good things will happen.
Back pain can be tricky. First off, anyone who’s ever dealt with it (pretty much everyone) knows it’s no fun. Second, there’s no overwhelming agreement as to what actually causes it. One person says weak glutes, another says tight hip flexors or hamstrings, and yet another may point to a bad hair day (NOTE: read this footnote, it’s a doozy —>).8
Third, if the stock photo I chose is any indication, back pain can also put a real damper on what can only be described as an Old Spice or Abercrombie & Fitch ad shoot.
In my career as a personal trainer and strength coach I’ve worked with hundreds of athletes and clients battling low back pain. It comes with a territory as a fitness professional. I’ve tried my best to arm myself with the best skill-sets possible (within my scope of practice) to help my clients work through their low back shenanigans. I can assess – not diagnose – and try to come up with the best game plan possible to address things.
And, to be honest, addressing one’s lower back issues can be mind-numbingly simple.
In short:
“Find what movements hurt or exacerbate symptoms, don’t do those movements, and then find movements that allow for a degree of success or pain free training.”
I’d be remiss not to mention Dr. Stuart McGill’s work here. Not only is he one of the world’s Godfathers of spine research, but he’s also one of the world’s best mustache havers.
He’s co-authored hundreds of studies and written several books on the topic of low-back pain – with Ultimate Back Fitness & Performance (now in it’s 6th Edition) and Low Back Disorders being his flagship pieces of work.
Speaking of Ultimate Back Fitness & Performance, look who makes a cameo appearance on pg. 289 in the latest edition.
HINT: It’s a bald strength coach whose name rhymes with Macaroni Flentilzore
For the Record: TG Life Bucket List
Get to a point in my career where Dr. Stuart McGill not only knows who I am, but emails me out of the blue and asks permission to use a picture of me in his latest book update.
Appear in a Star Wars movie.
Become BFFs with Matt Damon
My bedtime becomes 8 pm.
I’d have to say, however, that his most “user friendly” book is Back Mechanic. In it, he breaks down his entire method for “fixing” low back pain covering everything from spinal hygiene, assessment, corrective exercise, and strength training.
I’m not going to belabor anything, you can purchase the book and peel back the onion on his protocols (seriously, the assessment portion is gold).
I’ve noticed a trend in recent years, though. Dr. McGill has done so much for the industry and his work is so ingrained in our thoughts as fitness professionals that I feel the whole idea of “avoiding spinal flexion (sometimes at all costs)” has bitten us in the ass.
Yes, avoiding spinal flexion is a thing, especially if someone is symptomatic and flexion intolerant.9. It’s that point, though, “avoiding spinal flexion” that has gotten the best of us for the past decade or so.
We’ve done such an immaculate job at coaching people to know what “spinal neutral is” via prone planks, side planks, and birddogs, and then used strength training to engrain that motor pattern, that (some, not all) people transitioned into more extension-based back pain because they lost their ability to move their spine into (pain free) flexion.
Dr. Ryan DeBell discussed this phenomenon recently where he discussed his own back pain history. He started as flexion intolerant, trained himself into “spinal neutral,” (which is what you should do), started to avoid all flexion like an episode of Emily in Paris, and after awhile, extension-based movements & positions started to hurt…because he was locked into extension.
As a corollary, I see this quite often myself: someone comes in to see me and both flexion and extension based movements hurt. It’s so frustrating for the person and I can understand why.
My job, then, as the coach is to garner confidence and self-efficacy with my client/athlete and work with him/her on what I know tends to work….find movements that do not hurt and work from there.
Dr. McGill has his own version of the “Big 3,” or his go to exercises when first starting with a low-back person:
The Curl-Up (I.e., not a sit-up)
Side Bridge or Plank
Birddog
Even when we master those movements, which are often very challenging for people when performed right, I’ll stick with them for a couple of weeks and just up the ante with appropriate progressions.
Lets take the birddog for example.
Birddog w/ RNT
The band adds an additional kinesthetic component where increased stiffness or engagement occurs in the anterior core and glutes. Truthfully, it’s not uncommon for me to START with this variation so the person can feel what their limbs are doing in space.
Birddog – Off Bench
Doing the birddog off the bench takes away a component of stability (feet off the floor) and forces people to slow the eff down and learn to control the movement. If they don’t, they fall of the bench. And I laugh.
Your Spine, Move It!
Going back to the assessment for a quick second, it’s not uncommon for me to assess someone and to find that their spine doesn’t move. Whether it’s because of a faulty pattern or they were coached to avoid flexion at all costs (even when asymptomatic) it’s as if their spine is Han Solo frozen in carbonite.
One screen I like to use is a the toe touch drill. When someone bends over to touch their toes there should be a consistent curvature/roundness of the spine. Often, what I’ll see is more of a “V” pattern where they’ll bend over, but instead of seeing a nice curve I’ll see their lower back stay flat throughout the movement; as in zero movement.
This can be just as detrimental as anything else. It may or may not be a root cause of their low-back pain, but I know it’s a red flag I’d like to address.
Segmental Cat-Cow
Below is a drill I’ve been using more and more with my low-back clients. We’re all familiar with the Cat-Cow exercise, where you round and arch your spine moving through a full-ROM.
Cool, great. The human body is great a compensating, and unless you have a keen eye for detail it’s easy to assume that if someone can round and arch their back they’re good to go. But
But are they? Often, if you SLOW PEOPLE DOWN it’ll become abundantly clear that they may move well in certain areas of their spine (thoracic), but not in others (often lumbar).
Coaching them through the movement – point by point, segmentally – is a fantastic way to hammer this point home and to help nudge them to move their spine in a slow and controlled fashion.
Give this one a try with some of your clients. COACH THEM. This drill doesn’t require more than two passes (up and down) per set, for a total of 3-4 sets. Helping them understand that they are allowed to move their spine – assuming it’s pain free – is a sure fire way to set them up for long-term healthy spine success.
Final Note (Because, #douchebagswillbedouchebags)
To appease the hoity toity internet warriors, couch coaches, and fitness influencers who have never coached an actual person (let alone a ham sandwich) out there. All of this DOES NOT insinuate that I am not ALSO using regular ol’ strength and conditioning to address things. All of the drills showcased above are just entry-level ideas or starting points.
I’m actually a massive fan of introducing unloaded rotational and/or spinal flexion/extension movements into the mix as well as loaded exercises such as Jefferson Curls to help build more resiliency within the spine and the musculature that supports it. In addition I’ll introduce things like tempo deadlift and squatting variations, various hip/low back dissociation exercises (I.e., other hinging alternatives), as well as a consortium of single leg exercises to help build overall strength.
As I always like to say…
You need to lift shit to fix shit.
It’s usually not a one or the other scenario. Both sides of the spectrum (motor control strategies and lifting heavy shit) need (and should) be considered.
But I PROMISE I am going to 1) be brief, and more importantly 2) showcase why it’s important and why it will help you feel better, move better, perform better, and likely turn you into a Jedi Master Spartan Sex God of Minas Tirith.10
The reason I ask is because, ideally, you want to see a 360 or 3D expansion of your ribcage when you take a breath in.
In other words you want to see a little of everything move – chest, belly, back, sides, not eyeballs.
Unfortunately, for the bulk of people out there, this isn’t the case. Many tend to be just be
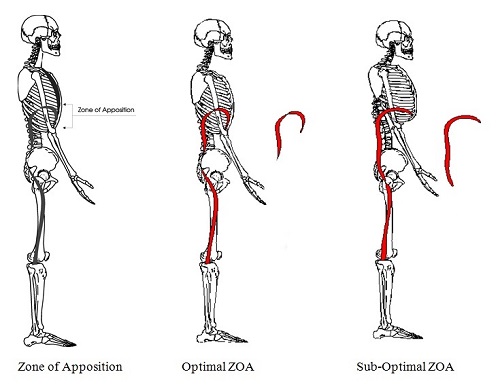
“chest breathers” or just “belly breathers,” and what ends up happening is a poor Zone of Apposition.
A Zone of Appo Come Again Now?
Zone of Apposition can simply be referred to as alignment. Or, more specifically, it can be described as the act of bringing together or into proximity.
Photo Credit: Postural Restoration Institute (<– AKA smart mofo’s)
If you take a gander at the Optimal ZOA picture (middle) you’ll see a diaphragm that’s domed out as well as aligned (stacked) above the pelvic floor; the ribcage is connected to the pelvis.
Conversely, in the Sub-Optimal ZOA picture (right), the diaphragm is flattened out and the ribs are in a more flared position; they might as well be located in Mordor in relation to the pelvis.
In non-nerd speak: Shit’s all out of whack.
At this point you may be thinking to yourself, “fuck outta here Tony. Who cares? Zone of Apposition sounds more like a term accountants use than anything I need to be worried about. Squats.”
Well, after listening to my colleague, Dr. Sarah Duvall, speak on the matter, here’s why it matters.
A Loss of Zone of Apposition Means:
Decreased core stability, control, respiratory efficiency, and exercise tolerance under fatigue…in addition to postural ramifications.
Increased accessory breathing muscle activity (scalenes, traps, levator), paraspinal activity, lumbo-pelvic instability, low back pain, SI joint pain, and even headaches.
A Quickie Breathing Assessment
Sit down in a chair and place your hands so that your fingers sit underneath and go around the sides of your ribcage.
Inhale.
What happens?
If an alien explodes out of your chest, that sucks.
You should feel LATERAL (into your fingers) expansion of the ribcage with a some motion in your chest and belly too. To steal another train of thought from Sarah, you should think of your breath as the handle at the side of a bucket.
As you take a breath in the handle should move out – LATERALLY – away from the bucket. This is a brilliant analogy for your ribs expanding.
Too, another overlooked aspect of the breath is what’s referred to as the High Hinge Point. This is the area that’s just underneath the bra line.
Can you (or your clients) expand air into this area.
Normal ZOA. Uncanny Jackedness.
Sub-Optimal ZOA (High Hinge Point). Still Uncanny Jackedness
Breathing into the back is an arduous and foreign task for many people, but it’s a key element to improving the ZOA.
Here’s a nice drill to help with that which I’ve used many times with my postpartum clients (as well as those attempting to resolve nagging low back or shoulder issues; encouraging the ribcage to move/expand works wonders for many people).
And That’s That
I suck at writing conclusions. To summarize:
1. Work on LATERAL rib motion.
2. Consider a high-hinge point in people and work to promote back-body expansion as well.
3. My wife and I bought the yellow chair on Wayfair in case anyone’s wondering…;o)
The topic of low back pain (LBP) – how to assess it, diagnose it, and how to treat it – can be a controversial one. I italicized the word “can” because I don’t feel it’s all that controversial.
Cauliflower as an option for pizza crust or Zach being chosen as the bachelor on the current season of The Bachelor (when it’s 100% clear that a ham sandwich has more charisma) = controversial.
Simple stuff to consider to help with one’s LBP = not so much.
The topic of low back pain and how to address it is controversial because there’s no one clear approach or answer to solve it.
(And if the last 3+ years of this pandemic dumpster fire has taught us anything it’s that we looooooove to argue over what’s best and what works).
SPOILER ALERT: Everything and nothing causes LBP.
Have ten different doctors or physical therapists work with the same patient and it’s likely you’ll get ten different opinions as to what the root cause is and what tactics need to be implemented to resolve it.
One person says it’s due to delayed firing of the Transverse Abdominus (TA), while someone else states it’s due to someone’s less than great posture or tight hamstrings.
For the record, all are weak excuses at best.
The culprit can rarely be attributed to any ONE thing.
But it’s amazing how often “tight hamstrings” is the fall guy.
Low back pain? Tight hamstrings.
Knee hurts? Tight hamstrings.
Have Type II Diabetes? Tight hamstrings.
Brown patches on your front lawn? Hamstrings.
It’s uncanny.
I mean, I could just as easily sit here and say in worse case scenarios LBP results from drinking too much coffee. I have zero evidence to back that up, but whatever.
…neither do most of the other “culprits” people tend to use as scapegoats.
So, why not coffee?
Or Care Bears for that matter, those sadistic fucks.
What works for one person, may exacerbate symptoms for someone else. And as my good friend, Dr. John Rusin notes:
“Fact of the matter is: there is NO one right way. it’s a big mistake to lump all LBP into the same category and even a bigger mistake to assume all of it presents the same or should be treated the same.”
There’s no way for me to write a thorough blog post on such a loaded topic; especially one that will make everyone happy.
It’s impossible.
I have better odds at surviving a cage match with an Uruk-hai.
Part of me feels like the proper response to the question “what causes low back pain and what’s the best way to address it?” is this:
Most people reading aren’t clinicians or physical therapists. There’s very little (if any) diagnosing going on in the hands of a personal trainer or strength coach. And, truth be told, if you are a personal trainer or strength coach and you are diagnosing, YOU……NEED…….TO…….STOP.
Just stop.
It’s imperative to defer to your network of more qualified (and vetted) fitness/health professionals whom you trust to do that.
However, it’s important to also consider we (as in personal trainers and strength coaches) are often the “first line of entry” into the medical model. We’re the first to recognize faulty movement patterns, weakness, imbalances, and bear the brunt of questioning from our clients and athletes when they come to us with low back pain.
There’s quite a bit we can do to help people.
What follows is a brief look into my mind and what has worked for me in the past with regards to LBP; a Cliff Notes “big rock” brain dump if you will.
Sorry if I offended anyone who likes Care Bears.
1) Rest Is Lame
My #1 pet peeve (and many agree with me) is that “rest” is the worst piece of advice ever.
“Go stick your finger in that electrical socket over there” would be better.
This isn’t to say there aren’t extenuating circumstances where taking a chill pill is absolutely the right choice; sometimes we do need to back off and allow the body a window of time to heal or reduce pain/swelling/symptoms.
That said, I think it’s lame when a medical professional tells someone to “rest,” or worse, informs them that they’ll need to learn to “live with low back pain.”
It’s a defeatist attitude and will spell game over for many people. Before you know it they’re living on a foam roller and thinking about a “neutral spine” while washing their hands.
(NOTE: I am not anti-teaching neutral spine to people. It’s a lovely starting point for most people, but at some stage people need to learn to move in (and out) of precarious positions…because that’s life).
A common theme reverberated in the S&C community is to say “strength is corrective.” I wholeheartedly agree with this sentiment. In fact, why the hell has this not been made into a t-shirt yet?
However, I think a slightly better moniker may be to say:
“Movement is corrective.“
We can use movement (and yes, strength) to help people get out of pain. Rest has its time and place, but I find stagnation to be more of a problem.
The body is meant to move and is wonderfully adaptive. And that’s the thing: adaptation and forcing the body to react to (appropriate levels of) change and stress is paramount to long-term success with LBP.
Sitting on a couch watching Divorce Court in the middle of the day isn’t going to help.
2) Move, But Move Well
I was watching Optimizing Movement with Mike Reinold recently and he noted there are three key elements to movement and why someone may not do it well:
Structural Issues
Coaching/Technique
Programming
It’s important to understand that, in this case, everyone is a unique snowflake.
Structure: Anatomically speaking there is huge variance amongst the population. Hip structure, for example, can have a large effect on someone’s ability to squat to a certain depth or get into certain positions. Likewise, who’s to say the hips are always the culprit? Even upper extremity considerations – like one’s ability to bring their arms overhead (lack of shoulder flexion) – can have dire consequences on back health.
The body likes to use the path of least resistance (also the most efficient) to accomplish any task. However in this case, “most efficient” doesn’t mean best. As Reinold notes:
“Efficient in this case refers to energy, not movement.”
Lack of shoulder flexion will often lead to compensation via more extension through the lumbar spine. It’s efficient movement, but it’s not better movement.
Coaching/Technique: I’m a firm believer that everyone should deadlift (it’s a hip hinge, learning to dissociate hip movement from lumbar movement, doesn’t mean we have to load it), but I don’t feel everyone should do it from the floor or with a straight bar.
Cater the exercise to the lifter, not the lifter to the exercise.
More on this below.
Programming: If someone lacks hip flexion why have them conventional deadlift? If someone lacks shoulder flexion why have them perform overhead pressing or kipping pull-ups? Some of the onus is on YOU, dear fitness professional.
Find what actions hurt or exacerbate symptoms, and stop doing it.
I know I just blew your mind right there.
For example:
1. Client says “x” hurts, and then places their body into some pretzel like contortionist position that would make a Cirque du Soliel performer give them a high-five.
Me: “Um, stop doing that.”
2. But that could also mean addressing how they walk or how they sit in a chair. Someone with flexion-based back pain, will like to be in flexion, a lot.
Maybe taking them through a slump test will offer some pertinent info.
Have them start in a “good” position:
Then, have them purposely “slump” into excessive flexion:
Someone who is flexion intolerant – despite preferring to be in that position – will often say this causes pain.
Ding, ding, ding.
So, the “fix” is to coach them up and try to keep them out of excessive spinal flexion. Cueing them how to sit in their chair and to get up (wider base of support, brace abs, chest up), building spinal endurance (and strength) via planks, and having them hang out in more extension may be the right path to take.
3. On the opposite side of the spectrum is extension, which is often a problem in more athletic populations and in those occupations requiring more standing (ahem: personal trainers/coaches).
Here you might put them into extension and see what happens.
Much like people who are flexion intolerant “liking” flexion, those in excessive extension will like to live in extension.
This will likely hurt.
Finding their spinal neutral is key too.
Hammering spinal endurance/strength via planks (done well) still hits the nail on the head, as does nudging them towards exercises that emphasize posterior pelvic tilt (much of time cuing people NOT to excessively arch during their set up on squats and deadlifts), and even drills that promote spinal flexion…albeit unloaded.
Spinal flexion doesn’t always have to be avoided. In fact, it’s sometimes needed.
Either way, meticulous attention to detail on finding spinal neutral – or pain from ROM – is huge. Once that is addressed, and symptoms has subsided, we can then encourage them to marinate in more amplitude of movement, taking them OUT of spine neutral (cause, it’s gonna happen in everyday life) and use the weight-room to help strengthen those new ROMs.
But I digress.
4) Don’t Treat People Like a Patient
I know this will rub some people the wrong way, but I still use the deadlift for the bulk of people I work with you have LBP.
Nothing sounds so absurd to me than when I hear someone say how the deadlift is ruining everyone’s spines.
To recap:
Deadlift = hip hinge.
Hip Hinge = learning to dissociate hip movement from lumbar movement.
Mic drop.
Resiliency is key in my book. And not many movements make the body more resilient than the deadlift or any properly progressed hip hinge exercise catered to the individual’s goals, injury history, and ability level:
Assuming I have coached someone up enough to understand spinal neutral and they’re able to maintain it, why not poke the bear and challenge them?
A deadlift doesn’t always mean using a straight bar and pulling heavy from the floor until someone shit’s their spleen.
I can use a kettlebell and band to groove the movement:
I can also use a trap bar, which is a more user-friendly way of deadlifting as it allows those with mobility restrictions to get into a better position compared to a straight bar.
https://www.youtube.com/watch?v=p-sA3PG1kGY
Too, I have found great success with various other exercises:
Farmer and Suitcase carries
Shovel Holds
“Offset” loaded exercises like 1-arm DB presses or 1-arm rows, lunges or RDLs (where you hold ONE DB to the side and perform the exercise). It’s a great way to increase the challenge to the core musculature.
Or even outside-the-box exercises like Slideboard Miyagi’s
So long as we’re staying out of precarious positions or those positions which feed into the issue(s) at hand, we’re good.
Find a training effect with your clients/athletes.
Help them find their TRAINABLE MENU.
And That’s That
People have low back pain for a variety of reasons: They’re too tight, too loose, too weak, have poor kinesthetic awareness, or they’re left handed.
The umbrella theme to remember is that there is never ONE root cause or ONE definitive approach to address it across the board. However, that doesn’t mean there aren’t some “big rock” things to consider that will vastly improve your’s and their chances of success.
NOTE: There’s only a few more days to get my latest continuing education resource – Strategic Strength – at $50 off the regular price. Today’s post discusses one of the main topics covered in the course: Assessment.
Assessment.
People don’t like the feeling of being judged – especially by complete strangers.
However, when it comes to working with a coach or personal trainer for the first time, an “assessment” is pretty much standard procedure; a means to an end with regards to collecting data to better ascertain someone’s starting point.
In Short: An assessment guides the coach to help figure out the safest and most efficient path for a client to reach his or her’s goal(s).13
That being said…I feel many of us are approaching assessment the wrong way.
I am not writing this as an attack against assessment
Likewise I am also not here to say one way or the other how you should assess your clients.
You know your clients/athletes better than I do.
I don’t care if your assessment of choice is the Functional Movement Screen, the Selective Functional Movement Assessment, PRI (Postural Restoration Institute), DNS (Dynamic Neuromuscular Stabilization), FRC (Functional Range Conditioning), whatever institutions like NASM or ACE prefer, or, I don’t know, duck-duck-goose.
Everything has it’s strengths and weaknesses.
More to the point, I would think that as people progress through their careers they’d take it upon themselves to actively change their minds the more they learn and gain experience.
They’ll experiment more and eventually “cherry pick” from several modalities to best fit their philosophy and approach to training.
Ideally “assessment” should be a smorgasbord of reaches, rolls, carries, squats, hinges, toe touches, twists, presses, and bicep curls (<— only half kidding on that last one), among other things.
Here is Gray Cook’s definition of assessment (a good one, mind you):
“In the assessment you take your education background, your professional wisdom, the particular situation, the time constraints, other historical information like a medical history or previous problems…and put all that together. That’s an assessment.”
Pretty hard to disagree with that, right?
Here’s my lame attempt:
“Can the person sitting/standing in front of you do stuff?”
I’m not tossing darts at everyone, but I do find that the bulk of fitness professionals out there use the initial assessment as an opportunity to search every crevasse (not that crevasse, get your mind out of the gutter), nook & cranny, and area of the body for “dysfunction.”
Many use the assessment as an opportunity to demonstrate to someone how much of a walking ball of fail they are.
“Okay Mr. Jones here’s what we got: your hip flexors are tight, you have forward head posture, you lack frontal plane stability, you lack ample scapular upward rotation, your left big toe has zero dorsiflexion, you have weak glutes, you’re quad dominant, your shoulders are slightly internally rotated, you’re probably gluten intolerant, your wife is cheating on you, and I’m about 37% convinced you have cancer.
If you purchase a 24 pack you’ll save $13 per session. Whataya say?”
Some of the above may be relevant and stuff you should focus on as a trainer. I mean, I’m not going to sit here and belabor a coach for wanting to improve a client’s thoracic spine mobility.
However, if I were the person listening to some laundry list of things I suck at or need to improve on, I’d be like………
………..”fuck off.”
Be Careful of Being Told to “Fuck Off”
There’s much I can wax poetic on when it comes to the topic of assessment. My biggest pet-peeve, though, is when coaches/trainers place waaaaaaaaaay too much emphasis on someone’s resting/static posture.
Lets revisit the picture from above.
Many high-end gyms implement this advanced form of “postural assessment” as an up-sell to seduce more people into purchase training.
Said individual stands in front of a giant gridded screen and is then hooked up with a bunch of probes and what not that are placed at strategic locations around the body that bloop and bleep.
It’s reminiscent of one the most terrifying movies I have ever seen, Fire in the Sky.
Remember that one?
You know, that alien abduction movie from the early 90’s where the main character is relentlessly poked and prodded by a bunch of aliens on their spaceship?
It’s terrifying.
Anyway, I can’t help but be reminded of that movie whenever I see someone being told to stand in front of a grid so some trainer can scrutinize every inch of their posture in the hopes they’ll be hired to “fix” it.
Who says it needs to be fixed in the first place?
I’m reminded of a photograph shared by Fort Worth, TX based physical therapist, Dr. Jarod Hall a few years back which hammers home my point.
Here’s what he said/posted:
“I want everybody to look closely at this picture and tell me what you see…”
“I see 20 of the world’s top athletes that have tremendous range of motion, strength, body control, and physical capacity… Yet all have significant variances in their static posture as determined by the holy grail plumb-line.
Static posture is near worthless to measure for injury or pain prediction.”
Placing all your eggs into one basket – in this case static posture, which a lot of fitness professionals do – is unfortunate.
Posture is a Position, It’s Not a Death Sentence
To steal from another really smart physical therapist, Dr. Quinn Henoch, “posture will always be relative to two things:
the task at hand
and the load
If you’re not taking into consideration those two things during an assessment – in addition to movement, repetition, speed, etc – and you’re only assessing people based off static posture, well, you’re not smart.
The question, then, is….”what should an assessment look like or consist of?“
Having the ability to extend the thoracic spine is a game changer for many people, especially for those who tend to be sequestered for hours on end in front of a computer on a day-to-day basis.
For lack of a better term, a lot of cool shit happens with extension:
The shoulder blades can retract and upwardly rotate.
It’s much easier to get the arms overhead.
It’s easier to keep the chest up during squats and deadlifts.
It makes for a “better” bench press. I.e., shoulder blades can retract and depress providing a more stable base of support.
The thoracic spine (thorax for the nerds in the room) is the “anchor” of the shoulder blades. Ideally we like to see congruency between the ribcage/thorax/t-spine/whatchamacalit and the shoulder blades.
When someone is a bit more kyphotic (rounded) in that area it makes it almost impossible for this to happen because the shoulder blades will often be more abducted and anteriorly tilted.
This can setoff a domino effect of other shenanigans such as a narrowing of the acromion space (for example), which in turn leads to rotator cuff issues, which then leads to not being able to bench press without pain, which, as we all know, means the Apocalypse is upon us.
Let’s avoid the Apocalypse.
To that end I’d like to take this time to share some of my “go to” T-Spine Extension drills I use with my own clients and athletes on a weekly basis.
1. T-Spine Extension Off a Foam Roller (Performed In a Way That Doesn’t Make Me Want to Swallow Live Bees)
Likely the most recognizable drill many gravitate towards – and for good reason (it’s a good one) – is T-Spine Extension off a foam roller.
However, many tend to go waaaaaaay too far with their total range of motion on this to where it becomes more of a lumbar spine movement.
Here’s how to do it correctly:
2. Prone T-Spine Extension
I reserve “fancy” for choosing a nice restaurant for a date night with my wife.15
I don’t feel the need to get fancy with my T-spine extension drills.
The Prone T-Spine Extension drill is a fantastic way to build mid-back endurance.
3. Child’s Pose Back Extension Off Med Ball
What’s great about this variation is that when we adopt the “child’s pose” (knees tucked underneath) we OMIT the lumbar spine.
So now the only area we can get movement is the t-spine.
4. Pigeon Stance w/ Reach Through & Extension
Taking the previous concept and upping the ante a little bit is this exercise I “stole” from Dean Somerset.
If we want to talk about a drill that provides a TON of benefit for our training buck this is it.
Here we get a stellar hip mobility/glute stretch, while at the same time taking the lumbar spine out of the equation (because that’s NOT where we want movement from).
Too, with the reach through (and then extension) we’re getting a double whammy effect of mid-back mobility goodness.
NOTE: I like to add in an inhale (through the nose) on the reach through and then a FULL exhale (out the mouth) as the individual extends back up.
NOTE #2: My tricep looks fucking amazing in this video.
5. Wall T-Spine Extension w/ Lift Off
This drill is a doozy as well.
Pushing the hips back and “settling” into your accessible t-spine extension ROM is money enough for most people. But when you add in the end-range “lift off” (lifting the hands off the wall) at the end, it adds that little “eff you” component not many people will like.
Be careful not to crank through your lower back on this one!
This one is more challenging than it looks, so way on the side of conservative when choosing the loads you use.
I’m using a 10 kg kettlebell in this video and am pretty sure I blacked out after shooting this video.
Want More Shoulder Magic?
Join me IN-PERSON for two upcoming Fall workshops I am putting on. I cover shoulder/hip assessment, programming strategies, the concept of the TRAINABLE MENU, favorite Decepticons, and much, much more.
It’s not lost on me that the title of this post will raise some eyebrows. The title shouldn’t be taken too literally, because I do feel there are ideal approaches, methodologies, and “rules” to consider when coaching any lift in the weight room.
That said, when it comes to exercise technique (or human movement in general) why are textbooks the metric at which we compare everything?
Textbooks provide context, information, and sometimes make for handy coffee table improvers.
However, we don’t live in textbooks. What a squat, sprint, overhead press (or hell, even a carrot cake) looks like in a textbook can (and usually is) a stark contrast from what is emulated in real life.
I do believe there are some universal tenets to coaching a deadlift or squat or bench press or kettlebell swing16 that will not only allow a client or athlete to marinate in its benefits, but to do so in a fashion that won’t increase their likelihood of injury (or their contributions to their physical therapist’s mortgage payments).
I’m interested in making people savages, but I’m also interested in the long-game. It wouldn’t bode well for business (or my reputation) if all of my client’s deadlifts looked like this:
To that end, with regards to universal tenets for deadlifting:
Loaded spinal flexion is a no-no.
That’s pretty much it.
If you’re following that one golden rule, you’re doing a better job than most. It’s sad, but true.
However, golden rule(s) aside, there are many intricate, more nuanced things to consider person to person. One’s training experience comes to mind. We can’t hold someone holding a barbell in their hands for the first time to the same standard as someone who’s been a competitive powerlifter for 17 years.
Likewise, someone with a vast and delicate history of lower back issues is not going to take the same path as someone with a “clean” health history. And, of course, other factors come into play such as goal(s), movement quality, favorite color, and anatomical/structural differences between individuals.
Someone with hips like this…
…is going to move differently – and presumably be coached differently – than someone with hips like this:
There are many, manyfantastic resources out there that help to break down anatomy, assessment, biomechanics, joint positions, and what’s considered ideal exercise technique. I have my biases as to what I feel is correct – as does everyone – but it’s important to take every resource with a grain of salt, because…
“Textbook technique only exists in a textbook.”
When I heard Mike Reinold say this sentence years ago my immediate reaction was this:
My second reaction was to start doing handstands down the sidewalk outside my apartment, but I didn’t.
You know, cause that’s fucking weird.
And because I can’t do a handstand.
Either way, what Mike said was/is 100% correct.
Textbook technique, in the real world, is every bit as much of a myth as detox diets making you pee rainbows or me riding a Dire wolf to work today
What we read or deem as “ideal” on paper, while often a great starting point for many people, doesn’t always translate to real-life. As coaches it’s important to understand this. Anytime we corner ourselves into one-train of thought or that any one thing applies to everybody, we’re doing the industry – and our clients/athletes – a disservice.
A Real-Life Example
A few months ago I started working with a woman who had been battling some low-back issues, yet wanted to hire me to take over her programming and help clean up her technique.
Specifically she wanted to hone in on her deadlift.
She was frustrated because no matter what she did (or who she worked with), her back always bothered her.
I like to be a fly on the wall and just watch people do their thing during an initial consult. I want to see what their default movement schemes are. In this case I set up a barbell on the floor, loaded it up with a weight I knew she could handle safely, and then asked her to do her thing. Her “default” stance was a conventional stance, and while it wasn’t the worst one I had ever seen, I could clearly see why her back may have been bothering her.
We had established earlier in her assessment that she lacked t-spine extension and her hip mobility wasn’t great either.
More to the point, after doing a simple hip scourand Rockback test, I surmised she was able to attain more hip flexion ROM with more hip abduction. An important point, as you’ll soon see.
Note: the Rockback test is a great assessment to use to figure out one’s “usable” ROM in hip flexion. The idea is to see if or when the lumbar spine loses positioning.
Bad Rockback Test
Notice when spine loses position.
Dead Sexy Rockback Test
Notice the spine stays relatively “neutral” throughout. Also, notice those triceps.
We can then compare what we see here with what we see on the gym floor.17
Going back to my client, she read a lot of articles and books on deadlifting, most of which told her that deadlifting = conventional stance. Always. Moreover, other coaches/colleagues she had consulted with in the past told her to use the conventional stance.
No exceptions.
This is what I mean by falling into the “textbook technique” trap. On paper everything sounds (and looks) great. Everyone can and should be able to conventional deadlift.
In real-life, though…not so much.
Here’s a before and after picture I took of my client. The top picture shows her original set-up with a conventional stance. The bottom demonstrates me putting her into a modified sumo stance.
Immediate improvement in her lower & upper spine position. Having her adopt a wider stance better complimented her anatomy, which then resulted in an infinitely better starting position to pull (no lumbar flexion, improved t-spine extension).
What’s more, with that modification alone she noted there was zero pain.
She left that session feeling motivated and hopeful about training. A win-win if you ask me.
I posted the above picture on some social media accounts – explaining much of what I mentioned above. And wouldn’t you know it: I was called out by a handful of coaches.
One stated the problem wasn’t with her anatomy, but that the real issue was my poor coaching. A funny assertion given he wasn’t in the room with me. Another coach agreed stating something to the effect of:
“No client has walked into “x gym” and not have been able to perform a conventional deadlift after a little coaching on day #1.”
I guess all I could have done at the time was to just go fuck myself.
I demonstrated I was able to clean up someone’s deadlift and do so in a way that was pain-free, and yet, here I was being told by a crew of All-Star coaches I had failed because I didn’t have her conventional deadlift. My actions, apparently, were on par with drop kicking a baby seal in the mouth.
Pump the Brakes
I hope people can appreciate the narrow-mindedness of this type of thinking. To expect everyone to fit into the same scheme or way of doing things because that’s what YOU prefer to do (or because a textbook told you to do so) is about as narrow-minded as it comes.
No one has to conventional deadlift.
Likewise…
No one has to low-bar squat or squat with a symmetrical stance.
No one has to bench press or bench press with an aggressive lumbar arch.
And no one has to start watching Severence on Apple TV. Except, yes you do.
I’d argue a “good” coach understands and respects that everyone is different, and that he or she will be humble enough to put their own personal biases in their back pocket and appreciate there is no ONE way to perform any exercise.