Before you move on, I wanted to let you know that Dean Somerset and I have just announced that we will be traveling to Dublin, Ireland this coming Fall to put on our 2-day hands-on workshop The Complete Fit Pro Blueprint.
It’ll be taking place the weekend of October 3rd-4th, 2026 @ Bodynamics in Dublin. We’ll be covering a lot of material from assessment and programming around injuries to more of the stuff most fit pros need more of…
Building systems to help you with time management and to make more money.
How to prevent burning out and to make more money.
How to build a brand and possibly a gym! (to maybe make more money).
How to better motivate your clients so that they’re consistent and to make more money.
And much, much more.
You can check out the full itinerary as well as register at the Early Bird price HERE.
WU-TANG!
Getting Strong(er) is Corrective
“Oh, I forgot to tell you…my previous trainer said I have a winged scapula, my left hip is a bit internally rotated, and that my posture isn’t great.”
This was less than five minutes into an initial assessment with a new client and it took everything I had to prevent my eyeballs from rolling out of their sockets. The snarky side of me wanted to say something like, “Oh my god, yes, I totally see it. Did (s)he also mention how your left ear is lower than the right? That’s messed up. We need to fix that.”
But I didn’t.
Nope, all I did was sit there, nod my head, listen intently, and kept repeating to myself “don’t stab yourself with this pen, don’t stab yourself with this pen, no, Tony, NO!”
People Think They’re Broken
It never ceases to amaze me how some people will harp on the most inane things when it comes to their body and performance and then regale me with stories of how their previous coach or trainer was a “corrective exercise specialist.”
I won’t invalidate their stories or experiences, of course, but it’s hard for me to listen to sometimes.
They’ll outline their “training” for the past few months (if not years), and it’s rife with positional breathing drills (which, for the record, I’m a fan of), postural stretches, and describe a foam rolling series that rivals the length of a Ken Burns’ documentary.
I’ll follow with “So, did you actually ever follow a strength training program consistently?”
“Yeah, sure, we did a bunch of corrective exercises and, after 19 weeks, we finally worked up to a bodyweight squat. I still have to work on my big toe dorsiflexion, though. Fingers crossed I can improve that by December.”
As an industry – and I’ll call myself out on this too (particularly early in my career) – we’ve done a splendid job at helping people feel like a bunch of walking balls of fail:
Your shoulders and upper back are too rounded.
Yikes, your pelvis is anteriorly tilted.
Oh…my…god…we need to work on your scapular upward rotation.
Shit, your FABER screen tested positive. How are you able to walk?
Also, FYI: you have Chlamydia.
It doesn’t surprise me in the least why so many people walk around thinking they’re fragile snowflakes who need to correct or “fix” everything before they do any appreciable training.
It’s our fault.
Strength coaches, personal trainers, physical therapists, athletic trainers, sherpas, we’re all culpable.
We can and need to do better.
And it starts with re-acquainting ourselves with what our main role as fitness professionals actually is…
…to elicit a training effect with our clients/athletes.
Again…Getting Strong(er) is Corrective
I say this with a grain of salt because “strong” is subjective, and can mean different things to different people.
Being able to deadlift 2x bodyweight is strong.
Being able to perform 15 pull-ups is strong.
Walking from Trader Joe’s to your apartment without putting down the bags is strong.
The ability to pull off wearing white after Labor Day is strong.
Doing whatever it is Cirque du Soleil performers can do is strong.
However, since I’m a little biased “getting stronger” in this sense – and more cogent to the conversation – refers to TRAINING.
I.e., lifting heavy things.
Unfortunately, many people have been led to believe lifting weights is dangerous. It seems you can’t go more than three clicks on the internet (or investigate certain certifications available) before being told barbells, dumbbells, machines, kettlebells, squats, deadlifts, high-reps, low-reps, and/or kittens are dangerous.
Who, me? Dangerous? Noooo. I mean, I’ll slit your fucking throat in your sleep if you don’t pay me any attention, but all in all….cuddles.
And just to set the record straight, and to push back with all my will to those people (worst of all, doctors, PT’s, etc) who keep spreading the message that strength training is dangerous (particularly when addressing a current injury)…
…I give you the LAWS of Loading:
Wolff’s Law – Bones will adapt to loads under which it is placed
Davis’s Law – Soft tissue will heal according to the manner which they are mechanically stressed.
For the “you only have one back” guy…is this then not why we train?1 Squats and deadlifts, when properly loaded and progressed, will do far more good for someone’s recovery from injury than most alternatives.
I hate the “everything makes you dysfunctional or causes dysfunction” crowd.
To which I say…the fuck outta here.
My friend Bret Contreras has the perfect antithesis to this faulty mindset:
“If you think lifting weights is dangerous, try being weak. Being weak is dangerous.”
And this is why I’m a firm ambassador in encouraging people to get strong(er), or more to the point, helping them figure out their “trainable menu.”2
Rather than pointing out everything that’s wrong with someone, I’d rather use the initial assessment (and subsequent training sessions) to highlight what they can do.
Lets use the classic example of someone who has “computer guy” posture. I.e., rounded shoulders, forward head posture, an affinity for pens.
When someone walks in exhibiting this posture a lot of trainers will write down a laundry list of stretches, thoracic (mid-back) mobility drills, and other “corrective” exercises to do.
Well, first, some will go out of their way to make the person feel like Cersei Lannister during her walk of shame.
I’m not opposed to utilizing corrective modalities to address postural deficits or mobility restrictions.
But I find when these sort of things are accentuated and serve as the “meat-n-potatoes” of a training program, it often sets people up for failure; they become more fixated on perfection at the expense of progress.
And lets be honest: NO ONE gets jazzed-up at the gym to do more T-spine extension drills.
I don’t want my clients to feel like a perpetual patient.
I want them to train, because training tends to be more palatable than Scapular Wall Slides. It helps people stay on task and not bored to tears.
And on that note, wanna know an excellent drill that helps nudge people into a bit more thoracic extension?
Kipping pull-ups.
FRONT SQUATS.
As you descend closer to the ground you have to “fight” to keep from folding over. In many ways the proper execution of the exercise itself is self-coaching; or dare I say, corrective.
If you don’t maintain thoracic extension the barbell rolls off your shoulders.
I may come across as the cantankerous strength coach in saying this, but I find more value in having my clients train – in a way that emphatically demonstrates success to them (by matching the programming to their goals and ability level) – than to corrective exercise them to death.
It’s not uncommon for people to seek out a coach or trainer because an exercise doesn’t feel right or because something – a shoulder, a knee, lower back, their soul perhaps – routinely hurts and they can’t seem to get out of their own way.
That’s where I come in to save the day.
Most of the time.
To fix someone’s squat technique and to maybe (probably) give him or her a reality check.
Boom or Bust
This is a term I stole from a friend of mine, Dan Pope of Champion Physical Therapy & Performance, and to a larger degree has its roots from a presentation I watched him do centered around the conversation of understanding shoulder pain.3
“Boom or Bust” refers to the person who handles their business as follows:
Train –> Do a lot –> To the point where it becomes painful –> Get pissed off, becomes upset, is inconsolable, and inevitably increase their volume of ice cream and Julia Roberts’ movies –> Feels better –> Repeat –> Cue face palm here.
I’m sure many of you reading – whether the above sequence of events describes you or some of your clients – can commiserate.
It can all be summarized using the following graph:
Again, props to Dan Pope. I essentially drew his graph, but added a little Tony LOLs.
What this depicts is a scenario and approach that keeps the alarm system sensitive as well as pain levels up. They train hard on Monday and hit their bench pretty aggressively, of course.
A day or two passes, the shoulder feels okay, and they decide to test the waters again and perform a bunch of high-rep push jerks. Another day or two passes, the shoulder starts to feel, normal again, and since they have zero fucks to give, decide it would be a swell idea to perform kipping pull-ups paired with handstand push-ups for AMRAP on broken glass.
All they do is perpetually plow through their pain threshold and the cycle continues over and over and over again like an episode of Russian Doll.
This, of course, is absurd, and makes zero sense.
Conversely, what also makes zero sense is the opposite approach…
…UNDER-loading, over corrective exercising people to death, or worse, doing nothing at all.
I’m not dissing the corrective component. Depending on how sensitive someone’s pain threshold is, we may very well have to resort to a myriad of side lying external rotations, arm-bars, and band work.
The key to improving pain, though, particularly with the long game in mind, is to elicit a smidge (key word: SMIDGE) of it during training. You want to tease it, buy it a drink, make out with it a little bit.
If you want to elicit change, you need to move. When we move, we induce something called mechanotransduction, which is just nerd speak for “tissue begins to heal.”
Pain, when DOSED ACCORDINGLY, can be beneficial during exercise. When we push into a little pain there’s generally better short-term results than if not. Think of it like this:
There’s a line in the graph above labeled “pain threshold.” On a scale of 1-10 (1 = no biggie, I got this and a 10 = holy shit, a panther just latched onto my carotid), exercise should hover in the 2-3 realm.
In this case, the person can tolerate things like push-up, landmine, and row variations.
When (s)he perform those exercises, the pain level never exceeds a “3.”
When (s)he’s done exercising, along with the hours after, the pain level never exceeds a “3.”
The following day, the pain never exceeds a “3,” and in an ideal situation is back down to baseline, which is a “1.”
That’s the sweet spot and what we’re after from a managing pain standpoint. We’re doing juuuust enough to elicit a training effect, playing footsie with the pain threshold, but avoiding any boom or bust scenario where we place commonsense ahead of our ego.
And then, over time, the graph looks like this:
I’m an idiot. That arrow pointing up should be labeled “Improvement in Pain.”
The pain threshold slowly creeps higher and higher, and before long, push-jerks, bench pressing, and fighting Jason Bourne ain’t no thang.
Training (with weights), when matched with someone’s current ability level, and when dosed effectively, can be corrective.
Want More of These Awesome Insights?
Dean Somerset and I are reuniting after six years (thank you COVID) to bring our latest IN-PERSON workshop to the masses. The Complete Fit Pro Blueprint will cover topics like this (and many, many more).
Boston – June 6th-7th, 2026 Dublin, Ireland – October 3rd-4th, 2026
I often speak on the importance of the test/re-test concept with regards to assessment.
It’s nothing fancy or elaborate.
You test something – whether it be range of motion or maybe a strength discrepancy – implement a “corrective” modality if something’s deemed out of whack, and then re-rest that shit to see if it worked.
The test/re-test approach helps set the tone for any future “corrective” strategies or programming considerations you’ll do as a coach or trainer.
In addition, and something I’d argue is equally as important, it also provides an added layer of value to the assessment.
If you’re able to demonstrate to someone a significant change or improvement in ROM or reduction in pain/discomfort by implementing a drill or two, and it’s something they’ve been struggling with despite countless interactions with other fitness professionals, what’s the likelihood they’ll bust out their checkbook or Bitcoin wallets (<—depending on their level of geekery)?
I suspect highly likely.
It demonstrates a perceived level of “mastery” and knowledge-base towards the assesser (you) and, in a roundabout, reverse psychology kind-of-way, delves into the “pain center” of the assessee (athlete/client).
In this example it can refer to literal pain such as a banged up shoulder, knee, or lower back. But it can also speak to pain in the figurative sense too. Someone who’s frustrated and “had it up to here!” that they can’t lose weight, or maybe an athlete who was cut from their high-school team would have a degree of “pain” that would incentivize them to take action.
Show someone success or a clear path of action, however little, and they’re putty in your hands.
Of course this assumes you’re not some shady shyster who tries to up-sell the benefits of some super-secret concurrent, 47-week, Eastern-Bloc training program you copied from Muscle & Fitness or, I don’t know, organic raspberry ketones laced with mermaid placenta.
People who promote and use smoke-and-mirror tactics are the worst.
But lets get back to the topic at hand.
Test/Re-Test
One of the main screens I use with my athletes and clients is their ability to lift or elevate their arms above their heads.
Shoulder flexion is important for everyone, not just overhead athletes and CrossFitters.
If someone lacks shoulder flexion, and they’re an athlete, it’s going to affect their performance. A baseball pitcher may be “stuck” in gross shoulder depression, which in turn will have ramifications on scapular positioning and kinematics, which in turn will result in faulty mechanics and compensatory issues up and down the kinetic chain.
Conversely, regular ol’ Hank from accounting, who likes to hit the gym hard after work, if he lacks shoulder flexion, he too could have numerous issues arise ranging from shoulder and elbow pain to lower back shenanigans.
Shoulder flexion – and the ability to do it – is a big deal in my opinion. And it’s a screen that should be a high-priority in any fitness professionals assessment protocol.
So lets say I’m working with someone who lacks shoulder flexion. I test it both actively (standing, picture above) and passively (on a training table).
I surmise that it’s limited and that it may be feeding into why a particular person’s shoulder has been bothering him or her.
I can use the test/re-test approach to see if I can nudge an improvement.
Now, as I’ve learned from many people much smarter than myself – Mike Reinold, Sue Falsone, Dr. Evan Osar, Dr. Stuart McGill, Papa Smurf, etc – you shouldn’t rely on any ONE screen/corrective.
Everyone is different, and what works for one person might not even scratch the surface for another.
With regards to addressing (lack of) shoulder flexion5, there are a handful of “go to” strategies I like to use.
And then it’s just a matter of seeing which one sticks.
1) Encouraging a Better Position
In order to elevate the humerus (arm) above your head, the scapulae (shoulder blade) needs to do three things:
Upwardly rotate
Posteriorly tilt
Protract
The ability to do so is vastly correlated with the thorax. Those who are super kyphotic (ultra rounded upper back) will have a hard time elevating their arms overhead. Often, the simple “fix” here is to foam roll the upper back and work on more t-spine extension and you’ll almost always see an improvement.
Bench T-Spine Extension
Side Lying Windmill
But what about the opposite? Those who are stuck in more “gross” extension and downward rotation?
I.e., the bulk of athletes and meatheads.
Here the shoulder blades can be seemingly “glued” down.
In that case some positional breathing drills to “un-glue” the shoulder blades (and to encourage more 3D or 360 degree expansion of the ribcage/thorax) would be highly advantageous.
All 4s Belly-Breathing
It’s amazing what a few minutes of this drill can do with improving shoulder flexion ROM, without having to yank or pull or “smash” anything.
2) Allow the Shoulder Blades to Move
Some people simply don’t know how to allow their shoulder blades to move. A prime example is this past weekend.
An attendee who’s a personal trainer – but also competes in figure – mentioned how her shoulders (especially her left) had been bothering her for eons, and she couldn’t figure out why.
We had her perform this drill.
1-Arm Quadruped Protraction
In reality, both protraction and retraction are occurring, but many people have a hard time with the former.
The idea here is to learn to gain movement from the shoulder blade itself and not via the t-spine.
Here’s another angle (because, triceps):
https://www.youtube.com/watch?v=eyNFNxqFlSc
After a few “passes” with this drill, she saw an immediate improvement in her ROM. What’s more, the following day when she showed up for Day #2, the first thing out of her mouth was “my shoulder feels amazing today.”
That’s a win.
3) Pin and Go
Another route to take is to have the person foam roll their lats. Not many people do this, and there’s a reason why: It’s un-pleasant.
I’ll have the person spend a good 30 seconds or so on each side and then have them stand up and perform a simple SMR drill using a lacrosse ball against a wall.
They’ll “pin” the teres minor down (basically, find the tender spot behind their shoulder and hold it there) and then work into upward rotation.
https://www.youtube.com/watch?v=9OiGt_O1FvY
Another five or so passes here, and I’ll re-test.
Many times I’ll see a marked improvement in their shoulder flexion.
Caveat
NONE of this is to insinuate that anything mentioned above will work for everyone. The idea is to understand that it’s important to “test” a number of modalities and then re-test to see if you find an improvement.
If you do, you’re likely barking up the right tree which will make your corrective approach and subsequent strength training more successful.
There’s a prevailing thought in the fitness industry – particularly amongst personal trainers and coaches – that everyone we come across is somehow broken or dysfunctional, and that in order to make things “right” we have to resort to an onslaught of endless corrective exercise protocols before a barbell is even looked at.
You know:
Band thingamajiggies.
Endless mobility drills and stretching.
Other stuff that makes me want to throw my face into an ax.
I am not downplaying the importance of “corrective exercise,” nor am I attempting to debunk the notion that it’s never useful or shouldn’t be prioritized. Sometimes more attention to detail with regards to one’s ability to access thoracic extension or, I don’t know, hip internal rotation, in order to accomplish a specific movement is warranted.
Sometimes people need “correcting.” (<— said in a creepy Mr. Grady voice from The Shining).
Whenever I start working with someone and they make note of how “x” exercise hurts “such and such,” rather than go down the corrective exercise rabbit hole and point out 27 different things that make them a walking, talking, breathing dumpster fire of dysfunction…
…I’ll do this novel thing, instead, where I ask him or her to perform the exercise and show me how they set-up and execute the movement.
Often, the culprit as to why something hurts or doesn’t feel quite right is the lowest hanging fruit like their setup and/or technique.
Let’s use the back squat as an example.
It’s not uncommon for many trainees to note how squats – barbell back squats in particular – tend to make their lower back feel like hot death.
Some fitness professionals like to keep things fashionable and will begin with an explanation that’s a bit more nefarious, if not altogether esoteric:
“Your lower back hurts when you squat because you lack big toe dorsiflexion, your left 4th rib is slightly rotated, and your chakras are all out of whack. See? Simple.”
First off: If this is how you talk to clients, you’re a tool.
Secondly: No one wants to listen to a laundry list of all the things that are wrong with them, and in doing so, does nothing but cement the idea that they’re broken and beyond repair.
Third: You’re a personal trainer not a physical therapist, act like one.
Fourth: Watch this video.
Those with a keener eye should be able to notice the difference between the two.
❌ TOP VIDEO
I initiate the descent by “falling” into my lower back.
In other words, rather than using the joints I want to perform the squat – ankles, knees, and hips – I recruit my lower back and use my spine for support as I descend towards the hole. Additionally, because I’m excessively arching my back (excessive anterior pelvic tilt) I’m increasing bone on bone contact as I go into deep(er) hip flexion, thus creating a more likely impingement scenario.
As a result, if you watch closely, I exhibit a bit of “butt wink” in the bottom because I’m running out of room in my hip.
As such my lower back HAS to come into play (even more) in order to go lower. To that end my back is basically saying “bye Felecia.”
By contrast, in the bottom video, I create more tension in my abs (creating a flexion moment) so as not to fall into (more) anterior pelvic tilt on the descent, and I think about squatting DOWN rather than BACK.
I’m still in APT, but using posterior pelvic tilt to nudge myself closer to “neutral.”
In Short: I’m improve my STARTING POSITION, which in turn keeps me more stable, the squat cleans up nicely (I’m able to squat deeper because I have more room in my hips), and the butt wink is all but gone.
More to the point…my lower back no longer hurt.
No need for a laundry list of correctives, stretches, mobility drills, or an exorcism.
All that was needed was to address my starting point (set up) and to have a better appreciation of the importance of TENSION.
To quote Denzel from Training Day: “King Kong ain’t got shit on me!”
In the last article – HERE – we looked at how we would address the issues that occur at the shoulders and thoracic spine. We discovered that optimal shoulder function comes from a healthy scapulohumeral rhythm, a mobile thoracic spine and humerus, and strong scapula and core muscles. In the end we identified common problems and proposed unique exercise solutions that can not only correct issues when they arise, but also strengthen the capacity of the joint altogether.
That followed my opening article in which I discussed my stance on the current state of our industry and how we’ve gone overkill in regard to corrective exercises. You can read that HERE.
Which brings us here to the next installment of the series – a similar dive into the lower back and hip joint, an anatomically different, but physiologically similar region of the body.
You’ll discover how lower back pain isn’t simply the lower back, how hip dysfunction or immobility requires more than flexibility and blood flow, and that integrated three-dimensional movements are the key to unlocking the hips and core.
As Shakira sings, “hips don’t lie”.
We are going to dive into the anatomy of the region, the physiology of the segments, and biomechanical implications that must be considered by any professional worth their salt.
We are going to unlock our, and our client’s, potential by adding another five great exercises to the equation too. But first, I want to take a moment to clear the air and amend a point I made in my previous post.
An Amendment on the FMS
In my last article I made a bit of a blunder when I described an issue that I have with the Functional Movement Screen. In my efforts to write a short, and interesting, piece of literature that covers a complex topic I did not effectively communicate my viewpoint on the matter. My claim that “the FMS puts the fear of God into trainers” isn’t quite accurate.
Brett Jones of FMS and I had a call on the matter and enjoyed an outstanding conversation on the FMS, how trainers are using it, and my specific area of concern.
Brett Jones (Note From TG: NEVER make Brett angry. Ever. Just kidding. Brett’s as professional as they come and one of THE best presenters I have ever had the pleasure of learning from. But seriously, don’t feed him past midnight.
He drew to my attention that the FMS, when taught properly and used properly, especially after the level 2 certification, provides trainers a lot of tools to correct and address issues that are present in the screens.
And he is spot on.
In my experience with the Functional Movement Screen, and the literature it publishes, I’ve found tremendous success in identifying, addressing, and correcting flawed patterns. The tools are present for a trainer to succeed.
So, to that end – the FMS itself is not an issue, and in fact, the certifications and resources that Gray (Cook) and Lee (Burton) provide are high on my list of recommended education for trainers. Simply put, much of the responsibility lays on the trainer performing the assessment to ensure they understand what they are screen, why they are doing it, and what it all means regarding the client’s exercise program.
And so, my point is really this:
“The FMS can put the fear of God in trainers who haven’t invested enough time to understand its purpose and nuance. This can be avoided by investing in your education and diving head first into new information.”
Basic Hip and Lower Back Anatomy – Skeletal
When looking at the skeletal anatomy of the spine and hip we find that it is quite simple. There are four major considerations:
The thoracic spine – capable of flexion, extension, and rotation. In an ideal world the thoracic spine handles the bulk or rotation and extension of the spine.
The lumbar spine – capable of flexion, extension, and rotation. In an ideal world the lumbar spine serves more as a stable base for movement that allows the pelvis to move underneath, and the thoracic spine to move above.
The pelvis – capable of anterior tilting (pouring water out of our belly button), posterior tilting (pouring water out of our back) and lateral tilts to either side (pouring water out of our sides).
The femurs – capable of internal and external rotation, flexion and extension, as well as abduction and adduction. Each of these movements are necessary to generate the variety of locomotion patterns we execute daily and for the specific movements we perform in training.
The ankle and foot are also capable of impacting health of the hips too, especially in the running community. Issues in these lower joints can cause negative effects to move upwards in the kinetic chain and begin causing negative adaptations in the hip joint or lumbar spine. We will address these correctives in the final part of this series, Hip-Knee-Ankle-Foot, so stay tuned.
For now, simply acknowledging their role in the process is enough.
Under the same principles, the shoulders can also impact the function of the hips. A dysfunction in the shoulders, such as upper cross syndrome, impacts the T-spine, which disrupts the lumbar spine and pelvis. Improving the health of the shoulder joint can help alleviate the poor postures that stress the lumbar spine and allow for a better functioning pelvis that experiences the ranges of tilt patterns because the lack of tightness in the lower spine. The scapula specifically should be considered (and will be in our correctives).
Basic Anatomy of Spine and Hips – Muscular
There are muscles that could be mentioned in this section that run very deep in the body and have very specific function.
The multifidus for example is a muscle that runs along the spine and has an important function; yet, our training practices aren’t exactly targeting it.
It is always good to know these types of muscles, such as the quadratus lumborum, obterus group, gemelli6 , and the aforementioned multifidus. Still though, this article is meant for our day-to-day efforts and most trainers simply don’t need to consider these things
There are some major players that you need to know though:
The abdominal wall, specifically the transverse abdominus, rectus abdominus, internal and external obliques, and psoas muscles. These muscles flex, extend, and rotate the spine and some act on the hip as flexors.
The gluteus maximum, minimus, and medius. These muscles act on the hip as external rotators and hip extensors.
The four muscles of the quadriceps, three muscles of the hamstrings, the tensor fascia latae as well as your abductors and adductors all act on the hip and knee joint. These muscles drive motion of the femur in the hip socket in a variety of ways that are unique to each pattern. In the next section we’ll isolate the specific motions and what muscles are involved for bookkeeping purposes.
The erector spinae, the quadratus lumborum, lattisimus dorsi, and lower trapezius muscles function on the thoracic and lumbar spine from the posterior of the body. These muscles are critical for putting the T-spine in the right place and stabilizing the L-spine during movement.
Basic Movement Physiology
Knowing what is in play is only half of the battle.
Note From TG:Goddamit Kevin. Rule #239 of being a nerd is that whenever the phrase “only half the battle” is used it must always be followed with GOOOO, Joe
In fact, knowing the structures and muscles involved is irrelevant if we don’t understand how they create movement in the body. To avoid blowing this article out into a thirty-thousand-word book on physiology we are going to have a down and dirty list of functions and the muscles that do the work.
I implore you to read and learn more about the muscular physiology that drives these movements from other resources. Play with things at the gym and try to “feel” what you can. I felt obligated to include this information in an honest effort to create the best free guide to hip correctives you’ll find. What you do with your education from there now rests in your hands.
Spinal Rotation or Lateral Flexion – Any of the core muscles mentioned above when functioning unilaterally. If one side of the rectus abdominus fires, then you’ll see lateral flexion and some rotation. Other rotators include the internal and external obliques and serratus anterior.
Hip Flexion – psoas major, iliacus, rectus femoris, sartorius, tensor fasciae latae, adductor longus and brevis, gracilis, pectineus. Some fibers of the glute minimus and medius engage here.
Hip Extension – glute maximus, biceps femoris, semitendinosus, semimembranosus. Some fibers of the glute medius engage too.
Hip Abduction – the glute maximus, minimus, and medius as well as the tensor fasciae latae. The piriformis functions when the hip is at 90 degrees.
Hip Adduction – adductor longus, brevis, magnus, pectinius and gracilis
Hip Internal Rotation – tensor fasciae latae, adductor longus, brevis, and magnus, pectineus, sections of glute medius and minimus
Hip External Rotation – piriformis, gemellus superior and inferior, obturator internus and externus, glute maximus, minimus, medius, psoas major, sartorius, quadratus femori
Now, I realize that this list reads like the appendix of a textbook, but don’t get lost in the noise. Notice the tremendous amount of overlap. You’ll see that the glutes have multiple functions as do the adductors and the TFL.
This sort of information at least shows us what the major players are going to be.
The Fascial Integration
We must also give attention to the intricate layers of fascia that are found in the core, hip, and thigh. Whether we address it through myofascial release or integrated non-linear movements, we must give it attention.
As noted in the previous edition, fascia is a highly communicative tissue that can arrange our body and its structures at a speed that is closer to the speed of light or sound than it is the speed of our cognition.
Fascia adapts, positively or negatively, to the stress placed upon it. Sit in a chair all day? Well, your fascia is likely bound up and dehydrated. Exist in a world where yoga, integrated movements, and sports are a major focus? Chances are you have healthy fascia.
The utilization of non-linear movements is one of the best ways of to improve fascia.
The Major Issues
The issues that occur at the spine and hips are almost always interconnected. A client could deal with just one or all of them.
Chances are that you’ll deal with all of these issues in some point in your career.
It is important to read and learn each of these as their own issue while also understanding that a client could show up to you with a Royal Flush of dysfunction. Luckily, the correctives we’ll discuss at the end are Swiss army knives – they are great for everyone.
1) Desk Posture
Once again, our lovely desk posture makes an appearance on the list. It is important to acknowledge the impact that upper cross syndrome (UCS) can have on core function, and thus hip function. If someone is slouched over with internally rotated shoulders, a kyphotic thoracic spine, and weak abdominal muscles, then we can very likely ascertain that their hips aren’t going to function optimally.
The lack of thoracic extension, poor function of the core muscles, and the overextension of the erector spinae and trapezius muscles dramatically impact the way someone can function up and down the length of their spine.
Ironically, many of these same flaws are also present in lower cross syndrome (LCS), which involves the muscles of the lumbar spine, abdominal wall, and the hips. Dysfunction caused from sitting all day can make the muscles involved weak (glutes and abdominals) or tight (muscles of the lower back and the hip flexors).
When a client presents these issues, especially together, it can be hard to prescribe any challenging exercises because their entire torso is locked from neck to butt. It is important to spot these issues early and begin implementing a corrective strategy that gets that client on the right path.
Thankfully, we’ll have some exercises below that will be great for both UCS and LCS issues.
2) Excess Anterior Tilt
When the pelvis is stuck in its “tipped forward” position for too long there are issues that can present themselves at rest and during exercise. In fact, continuing to exercise, especially with exercises that promote even more tilt, can cause damage to the vertebral discs.
In this position the erector spinae and QL are pulled tight while the anterior core is left in a lengthened and overstretched state. This sort of weakness in the abdominal wall makes optimal hip function harder to achieve and can lead to injuries at the spine.
Another unfortunate consequence is the overextension of the spine, or flaring of the rib cage, which can create the appearance of a midsection that is holding excess bodyfat. This bulge is simply a result of poor posture and would disappear once the pelvis is set back to neutral.
It should be noted that though that the pelvis should be able to anterior tilt through a full range of motion – it just shouldn’t be stuck that way.
3) Excess Posterior Tilt
The exact opposite of anterior tilt is the posterior version, which is when the pelvis is tilted back too far. This “belt-buckle to nose” condition is often found in individuals with lower cross issues since their abdominal walls are weak and their hip flexors overactive.
This position pulls the glutes completely in line with the body and flattens out the lumbar spine by ridding of the natural curvature of that region. This is not only “less attractive” due to the appearance of having no ass, but it also dangerous to load someone who can not achieve even low levels of hip extension and hip flexion. When someone is stuck here – they effectively have no idea of how to move their hips.
The corrective strategy here requires specific interventions that improve the awareness of the client as well as the strength of the glutes, hamstrings, abdominal wall, and even latissimus dorsi muscles. Additional efforts can be spent to improve external rotation of the femur and abduction too.
Once again, the hip should be able to posterior tilt during some movements and to help create stability.
4) Sticky Femurs (no, this isn’t technical)
One of my favorite terms for someone lacking the ability to rotate their femurs in their hip sockets (internally or externally) is “sticky femurs.” What I mean by this statement is nothing more than the image of having gum stuck in the joint that prevents optimal movement.
This is a combination of a lack of mobility in the joint due to not experiencing enough movement variation. Very active people could have “sticky” hips if they don’t cross train or experience movements in all three planes. Many “big” lifters struggle with external and internal rotation at the hip.
The other side of the coin is weak external or internal rotators that are incapable of owning the position that we put the femur in with excellent mobility. This is very common in dancers, those who practice yoga, or others who don’t actively strengthen these muscles. Detrained individuals fall into this category too. The mobility is there, but strength at end ranges is not.
5) Poor Coordination
Sometimes the issue is simply getting people to start exercising more and feeling their body move in a variety of ways. Frequent exercise, especially when done with coordination as the end goal, can improve a lot of functions of the hips on its own. It is amazing just how bad things can get when someone is rusty or de-conditioned.
Of course, you’ll need to spend time mobilizing and strengthening the various elements of the hip joint, but you’ll likely see increased output by simply exposing clients to new forms of movement and exercise. Any training program that features unilateral, contralateral, ipsilateral, and bilateral movements in all three planes is ideal.
6) Weak Core
Lastly, poor strength in the core itself can cause serious issues. It can derail any segment of the body since the primary function of the core itself is force transduction – AKA – translate forces from the limbs to each other and to the external environment.
A strong core is capable of remaining stable as the limbs create and accepts force. We must ensure our clients can move through all three planes of motion, with optimal function at the joints, with a variety of loads and challenges, because they possess a strong core. For this reason, most of our programming for the core should emphasize creating, and maintaining, tension.
The Corrective Exercises
Once we dive into the corrective strategies it is important to acknowledge that all these movements can be used to help with each issue. All these movements in some way will impact the ability of the client to succeed in overcoming hip dysfunction.
Each are also excellent in isolation as warmups, isolated correctives, and “fillers” between primary movements (as Tony often discusses). The Sumo deadlift, obviously, is a primary movement that should occur early in a program, especially if we are loading it up.
1. Glute Bridge Pullovers
https://www.youtube.com/watch?v=744uVr_qbqM
This simple variation of the traditional glute bridge accomplishes two major things:
Drives all the major benefits of the traditional glute bridge
Incorporates lat tension into the glute bridge – a key point for deadlifts and squats
You can strengthen the lats, glutes and abdominals while also addressing coordination issues. This exercise can help with every problem listed above except for “sticky femurs.”
2. Foot Elevated Glute Bridges
https://www.youtube.com/watch?v=uB_OanZw_Js
Another glute bridge variation that can dramatically improve the strength of the hip muscles (both flexors and extensors). By elevating the feet, you can increase the range of motion you’ll experience and improve your ability to drive into the bridge.
The key is to manage the lumbar spine and avoid overextension. The sort of exercise is great for strengthening the core, improving pelvic tilt issues, addressing coordination, and improving posture.
3. Cossack Squats
https://www.youtube.com/watch?v=XC0InYzYb00
A highly advanced variation of a lateral squat – the Cossack squat asks for an incredible amount of external rotation from the femurs. It targets the muscles that drive abduction and hip flexion and extension while moving through the frontal plane.
You can use your arms to help counterweight your body as you go down and find depth. Ease into the motion and look to improve your depth and mobility over time. This is an advanced exercise that can be regressed to holding onto something like a squat rack to help with weight transfer.
4. Copenhagen Side Planks
For some reason we love naming exercises after places – this side plank variation being no different. However, this is one of the most incredible ways of working the adductor grouping without needing to add external load. You’ll also integrate your internal rotators and the muscles of the rotary core. This sort of combo lends itself to improving strength and coordination.
Your goal should be to squeeze the bottom leg towards the bottom of the bench without rolling over and dumping the tension in the side plank.
Drive yourself to maintain an ideal side plank posture the entire time.
5. Loaded Marching Carries
https://www.youtube.com/watch?v=JuHCDH1T43E
Loaded carries are a movement pattern all their own. Few things can rival the simple effectiveness of grabbing heavy weights and walking around with great posture. This variation though, greatly improves the function of the hips by incorporation intentional hip flexion through the march.
Focus on driving the knees perfectly vertical, play with your speeds, and always emphasize a tight upper back, strong core, and depression of the scapula.
This exercise addresses every single problem mentioned above.
6. Sumo Stance Deadlifts
https://www.youtube.com/watch?v=XhxviMQEWOM
The validity of a medicine is always in its dose. Sumo stance deadlifts are one of the best corrective exercises you could program assuming:
You or your client are ready for the stress of loaded hinges
You choose the appropriate version for where you are in your training routine
You have earned the right to be here by exercising pain free with less aggressive modalities.
The reason that the sumo stance is so great is that you are literally working all of the muscles of the thigh, hip, core, and upper back at the same time. The external rotation and abduction of the femurs improves the strength of the muscles involved while also helping clients discover new mobility and neuromuscular coordination. This pattern is especially useful for those who spend most of their days sitting.
7. Loaded Beast to World’s Greatest Hip Opener
https://www.youtube.com/watch?v=spt_l-XhZRE
An interesting cross between a traditional mobility exercise and one of the loading phases in Animal Flow – this is one of my go to exercises for increasing the dynamic ability of my clients.
This version allows you to go fast or slow depending upon skill set while also loading the hips through a full flexion and extension cycle, improving coordination, and integrating the upper body and lower body together in a mobility movement.
You can use this as a “energy system” filler if you so choose (and your client is ready).
BONUS:
8. Hinge Position Face Pull
https://www.youtube.com/watch?v=JibVKRxbgAs
A lot of clients need help discovering how to hinge. Those same clients also struggle with maintaining tension in their cores and lats too. This exercise combines an active movement of the shoulders (great for shoulder health) with a passive hip hinge to improve core and hip strength.
Add this into any of your programs as a variation of the face pull that challenges your clients do more than just yank on the cable.
Wrapping it Up
Your ability to improve your client’s function around their hips depends on your ability to address the mobility and stability needs of the segment while also ensuring they are getting enough of a training stimulus to cause change. Understanding the nuances of the anatomy and physiology is a critical step in developing progressive programs that correct issues and cause a training effect.
The final part of the series will discuss the relationship of the hip-knee-and ankle.
I already wrote similar posts covering how I implement fillers with deadlifts and squats, so it only makes sense to finally follow suit with something discussing the bench press.
As a quick refresher for those first tuning in: “Fillers” are low grade exercises that address a specific mobility or stability issue – lack of glute activation, tight hip flexors, poor scapular upward rotation, as examples – which are performed during rest periods of a main exercise.
Fillers could also be a simple stretch.
In short the idea is do something productive during your rest periods – other than stalk your ex on Instagram – that’s not going to affect or deter performance on subsequent sets of deadlifts, squats, bench presses, and the like.
Another way to look at it is this: I know it, you know it, your parent’s mailman’s second cousin’s godfather knows it, we all know it…
…you’re (probably) going to skip your warm-up.
Fillers are the compromise.
Instead of giving people a laundry list of warm-up drills they’re not going to do, I’ll sprinkle fillers in as PART OF THE PROGRAM.
So in no particular order here’s a quick-n-dirty rundown of some of my go to fillers on bench day.
1. Rows
Okay, I’m cheating a little bit here.
I’m only speaking for myself, but I find rows are something most people can’t include enough of in a program. Many of us are so overdeveloped and/or tight in our anterior chain – namely pecs – that it’s not uncommon practice for me to pair a rowing variation with EVERY set (including warm-ups) of bench press to help offset the imbalance
I don’t care if it’s a DB row, Seated Cable Row, Chest Supported Row, Seal Row, TRX Row, Face Pulls, or Band Pull-Apart…I want some kind of row tethered to every set of the bench press.
And then I’ll include 1-2 more rowing variations later in the session too. The whole notion of a balanced approach to program design – where you attempt to include a 1:1 (press:row) ratio – while noble and good place to start, tends to be a bit underwhelming.
I’ll often say it’s more beneficial to UN-BALANCE someone’s program (to the tune of 2-3 rowing variations for every press) to to better “balance” them.”
So, as more of an umbrella theme to consider, just staying cognizant of rowing volume (and adding more of it into someone’s program) is going to be leaps and bounds more effective for long-term shoulder health and training domination than the litany of correctives that can be substituted in.
2. Band Posture Corrector
This is a drill I stole from my good friend and strength coach Jim “Smitty” Smith of Diesel Strength.
Sitting at a desk all day, every day, can be brutal.
The muscles on the back side (namely, rhomboids) get long and weak, while the muscles on the front (namely, pecs) get short and overactive.
A good bench press requires a fair amount of scapular retraction and depression to help protect the shoulder joint and to provide a more stable “surface” to press from.
This drill targets those muscles involved.
Simply grab a band, loop it around your shoulders, and “reverse” the posture.
I like to perform 10-20 reps with a 1-2 second hold on each rep.
3. Foam Roller Snow Angel
Likewise, the bench press also requires a decent amount of thoracic extension (which makes it easier to retract and depress your shoulder blades).
The Foam Roller Snow Angel allows for a few things to fall in place:
A nice pec stretch.
Nudges more thoracic extension (by lying on the foam roller).
I like 10-12 reps here.
4. Child’s Pose – off Med Ball
Pigging back off the above drill, this one also helps to improve thoracic extension in addition to strengthening the scapular stabilizers when you add a static hold at the top of each rep.
Adding the medicine ball into the mix along with flexed hips helps to keep the lumbar spine out of the equation.
Excellent strength coach, and outstanding Canadian, Dean Somerset once stated in an internet post, or maybe it was a blog, “there is always a cost of doing business.” He meant it as a point of emphasis when talking about the various effects of training programs and specific exercises. But he also could have extrapolated it outwards to reflect the stresses of our daily lives.
Poor posture while seated for twelve hours is going to have a cost associated with it just as German volume training.
Note From TG: OMG, German Volume Training brings back the worst memories. I don’t know which was worse: getting kicked on the balls or GVT?
For this reason, the fitness industry has made a major shift towards corrective exercises. Once seen as the tools of progressive physical therapists – these mobility, stability, and integrated exercises have become critical elements in training programs for elite athletes, nimble geriatrics, and the average Joe and Jane alike.
The growth of corrective modalities in conventional personal training is a good thing overall. However, as I pointed out in the introduction to this article series – HERE – there exists a very big downside to the obsession with movement perfection and body correction.
There needs to be a better way of correcting people’s movement flaws, overcoming their specific weaknesses, and getting them to a place where they can safely train hard. Far too many coaches are “under-training” their clients because they are investing too much time “correcting” things. At some point we need to get people training hard towards their actual goals.
Using Your Head For Their Shoulders
There may be no part of the body more susceptible to under-training than the shoulders. With multiple skeletal structures, a bunch of muscle attachments, and a relationship with the spine – there are a lot of reasons that someone wouldn’t be “allowed” to train hard with their shoulders.
Training them includes more than the traditional bodybuilding approach too.
The glenohumeral joint is involved in all upper body pushing and pulling motions as well as the specific isolation exercises that are popular in bodybuilding programs (such as lateral raises or chest flyes). The scapula and clavicle are too, but their positioning on the body also impacts movement such as the deadlift and squat.
Because of their high level of integration with every exercise we do, the shoulders are often the most banged up part of a client’s body. Our poor postures and ill-advised training programs aren’t helping us. Often the two compound each other and only worsen any dysfunction that exists.
Hence the need for correctives.
Really though, the shoulder itself is a bit of a miracle joint – with all the muscles that cross it, the fascia, the nerves, blood vessels, and obvious skeletal structures – it is amazing that it functions as well as it does.
But there can be a whole host of issues going on, or there can be just one. And that is what is most challenging about assessing and correcting shoulder dysfunctions.
It could be as simple as improving someone’s ability to retract and depress their scapula, such as when someone’s posture isn’t where we’d like it.
Or as complex as improving external rotation of the humerus while also stealing more extension from the thoracic spine and stability from the scapula during upward rotation and elevation, such as when a client wants to get better at pull-ups.
No matter how intense the problem is it is important that we as coaches keep our processes simple.
Removing the Restrictions
Yet, simple is not how most coaches approach shoulder health.
In fact, if you were to follow many of the conventional prescriptions that are floated through the industry, then you’d avoid many of the things that produce big results for your clients in favor of small correctives that make small changes. While some clients do need more intervention with these corrective methods – most simply need enough to create an opportunity for more intense training.
If you were to follow many of the guidelines that accompany something as notable as the Functional Movement Screen (the FMS), then many of your clients would not be allowed to press, or pull vertically, or load up abduction or adduction in the frontal or transverse planes until they were able to get a “2” on the shoulder mobility assessment.
While Gray Cook and Lee Burton did an incredible job creating a screening tool that helps coaches discover dysfunction and lack of movement prowess – they also created a system that is preventing a lot of clients from actually getting better.
Note From TG: For anyone interested (I.e., everyone) I wrote about my experience taking the FMS and what I took from it HERE.
The protective measures and governing principles of systems put the fear of God in personal trainers who use them. Many are afraid of loading anything until they see a two on the scoreboard. It is a steady dose of low intensity or no intensity correctives until that day.
Which is where the problem with corrective exercises starts:
Low to no intensity corrective exercises aren’t why clients improve over time. Instead, it is the strengthening exercises that come after these correctives that matter most.
If we are to improve how we utilize corrective exercises in our programs, then we must be willing to accept that what we now know isn’t perfect. We must be willing to entertain the idea that there is a better way of doing business. It is this exact mentality that drives innovation in technology.
It will drive innovation in fitness if we let it.
—-
(It is important to pause here and make a statement – this article is not meant to treat, diagnose, or prescribe methods or modalities for someone who is dealing with diagnosed injury or dysfunction in their shoulders. Traumatic injuries, conditions such as frozen shoulder, cervical kyphosis, and others require a finer touch from qualified medical professionals.)
If Not This, Then What?
Corrective exercises are like the bore that drills tunnels in the side of a mountain. They create the space for the construction to take place, but they aren’t the construction. You wouldn’t want to drive through a tunnel that hasn’t been reinforced with steel supports and millions of pounds of concrete, so why do you think that corrective exercises are enough to create a finished product in fitness?
The mobility and stability exercises that we define as “correctives” simply create the space for more optimal change to take place. They create the opportunity for well-selected strength exercises to change the tissues for the better.
For shoulder health we find that the classic approach of wall-angels, thoracic roll-overs, and cat-cows are simply creating the opening for which exercises like loaded carries, supinated pulldowns, and banded retractions fill with strength and stability. Our goal needs to be to do enough to get to the exercises that stimulate adaptation and create positive change; in the shoulders and in the rest of the client’s body.
Our responsibility as trainers is to help our clients overcome dysfunctions and improve their movement quality – sure. But our job also implies that we help our clients burn calories, build muscle, and come just short of conquering the universe.
Before diving into the actual corrective exercises that will open the gates for us to train with the intensity our client’s want and need, let’s ensure that everyone reading is on the same page on the anatomy and physiology of the shoulder joint.
The Basic Anatomy and Physiology – Skeletal
When looking at the shoulder joint you are presented with three major bones: the clavicle, the scapula, and the humerus.
The clavicle (or collarbone) is the most stationary of all of these structures, but its lateral aspect does elevate and depress in reaction to movements of the other bones. The humerus, the upper arm bone, is designed for external and internal rotation within the socket – known as the glenohumeral joint.
The humerus can move through flexion, extension, abduction and adduction, and horizontal abduction and adduction by rotating around the glenohumeral joint in each of the three planes (sagittal, frontal, transverse). These movements are aided by the function of the scapula.
The scapula (or shoulder blade) is the large bone in the back of the body. It is capable of six motions: elevation, depression, upward rotation, downward rotation, protraction, and retraction. These movements are also correlated to the three planes of motion too – sagittal, frontal, and transverse respectively.
The spine is also involved in shoulder mobility and stability is often left out when looking at function. We will explore this relationship in the next section when we begin looking at how core function can impact shoulder mobility as well as how thoracic extension is necessary for optimal function of the shoulder joint.
The Basic Anatomy and Physiology – Muscular
The human shoulder functions as incredibly as it does because of the incredible number of muscles that are involved. Some control the humerus, others control the scapula, and others control the spine.
Most of these muscles are found in the back.
When looking at the muscles that contract at the shoulder, we must separate the muscles that control the external rotation and internal rotation of the humerus from the muscles that create the six motions of the scapula. While some muscles share functions – it is important to identify its primary action and what it acts upon in order to better understand how the shoulder wants to function.
The four muscles of the rotator cuff are most responsible for the external and internal rotation capacity of the humerus.
There is evidence to support that the triceps are involved in external rotation, especially under load (just turn your arm around as far as you can right now, and you’ll feel the lateral head of the triceps contract). Therefore, the triceps join the supraspinatus, infraspinatus, and teres minor as external rotators of the humerus.
With that claim we can also ascertain that the biceps and pectoralis group are involved to some degree in internal rotation (although there is significantly less IR available at the shoulder joint). The subscapularis is the internal rotator of the cuff.
When examining the muscles that move the scapula, we are simply looking at the muscles of the upper back; the lats, teres major, rhomboids, trapezius, levator scapulae, the serratus and the three external rotators of the cuff. Each of these muscles have specific functions on pieces of paper, but it is imperative as coaches that we realize that most exercises performed in a gym setting involve more than just one of these muscles doing one of these functions.
It is easy to point at the traps and say “oh, they are elevators and contribute to upward rotation.” It is less easy being able to look at a flawed motion and know exactly what is wrong:
For example, many coaches will point at someone having issues with retraction and think “ah, the upper traps are overactive and the teres major/minor need strengthening.” They could be right and probably are in a population of people who sit with rounded thoracic spines and internally rotated shoulders.
Add in forward neck and shrugged shoulders and this “diagnosis” seems spot on.
However, getting just the teres group to fire without activating the infraspinatus or supraspinatus is nearly impossible in a traditional training setting. Getting someone to stay out of their upper traps sounds like a great coaching cue, but that requires getting them to fire the muscles that contribute to scapular depression; the lower traps, pectoralis minor, and latissimus dorsi at the same time – something most clients (or you) can’t do consciously.
In fact, a lot of scapular depression comes from the ability to put the thoracic spine into extension. Doing so involves activation the lowest fibers of the traps, the lats, the upper abdominals, and a whole host of muscles that are so deep and connected to the individual vertebrae that considering them in training is pointless.
When these muscles contract and thoracic extension takes place, you find that the scapula better slide into the depressed position.
The Core Connection
Yet, thoracic control isn’t completely isolated either.
It is very hard to contract the thoracic muscles without some level of core control. In this instance, the core includes the anterior muscles of the core that we know (rectus and transverse abdominals, internal and external obliques, and Psoas Major.
It also includes the muscles of the posterior core: the quadratus lumborum and the erector spinae.
Conscious contraction of these muscles allows for the core to hold tension, which better stabilizes the lumbar spine, which better allows the thoracic spine to go into extension, which better allows the scapula to depress, which better allows the humerus to externally rotate. As you can see, everything is connected, which is why we can’t use such generic correctives to solve complex problems.
A Less Important Factor?
You’ll notice that we haven’t yet mentioned the deltoid – the most known shoulder muscle. For all the attention it gets in bodybuilding circles its function is not as critical to shoulder function as you’d believe. The anterior fibers assist in internal rotation and drive flexion of the arm while the posterior fibers aid in external rotation and initiate horizontal abduction. The lateral fibers function to create abduction of the arm in the frontal plane.
From a corrective standpoint, it is very rarely an issue with the deltoid that proves to be the problem. In fact, it is often the overdevelopment of the deltoids and upper traps and underdevelopment of the rotator cuff muscles that create impingement issues in dedicated lifters. Great corrective exercises keep the deltoids involved and avoid shutting them out.
The Hidden Gem
In recent years we’ve come to learn that the fascia in our bodies is more than just a covering and more than just extra tissue that gets cut through in surgery. It is a living tissue that is involved in our function on a day by day and minute by minute basis.
In fact, research from Michol Dalcourt and the team at the Institute of Motion have proven that the fascia can communicate information across the body faster than any muscle tissue. Its ability to compress and expand is crucial for athletic development.
Unfortunately, many fitness professionals see it as tissue that is addressed with foam rollers, lacrosse balls, and other release methods. This isn’t wrong of course as these implements can do well to increase blood flow, increase hydration of the fascia, and improve mobility of the joint in question. However, we can also train our fascia just as we train our muscles. We must look to incorporate the variety of slings that Thomas Meyer’s discusses in his text Anatomy Trains.
In our solutions section we’ll explore a few ways to do that to improve the function of the shoulders and truly correct any issues that exist.
But first, we must identify a few of the most common problems.
Common Problems
1) Desk Posture (UCS)
The most common problem that a client will present in regard to their shoulder health is the classic “desk posture”. The scapula sits in protraction and elevation while the humerus’ are internally rotated. This posture is held for eight, ten, and twelve hours a day. Over time the pectoralis muscles get tighter, the trapezius muscles lengthen, the muscles of the scapula and glenohumeral joint get weaker, and the client continues to worsen.
The most advanced form of this condition is known as Upper Cross Syndrome (UCS) – a severe condition of immobility that usually involves additional intervention with physical therapists, and sometimes, orthopedic surgeons. This posture often presents forward neck as a well – a dangerous condition of the cervical spine.
The treatment for individuals in this position is to correct their posture and work to move them in better retraction, depression, and external rotation. However, many of the common methods do not provide enough intensity to stimulate muscle growth or strength adaptations in the muscles of the upper back. It is crucial for trainers to invest time in building their clients upper backs and coaching optimal patterns if the corrective interventions are ever going to stick.
2) Poor Scapulohumeral rhythm
For many people the pain they experience in their pressing and pulling motions is a result of a poor pattern being present. Of course, there are others who have legitimate issues such as shoulder impingements, strained muscles of the rotator cuff, or overactive trapezius muscles that make doing certain movements nearly impossible. The rest though, simply need help reworking their patterns and an emphasis on strengthening the muscles that control those patterns.
The scapulohumeral rhythm refers to the quality of movement that occurs when we consider the scapula and glenohumeral joints interaction. People with great rhythms typically an exercise pain-free while people who lack control and patterning struggle to accomplish even the most basic tasks.
This topic is quite deep, but in short realize there is a relationship between the position of the humerus and where the scapula “should” be.
For example, in a traditional dumbbell overhead press the scapula should be upwardly rotating and elevating as the humerus adducts towards the midline at the top of the press. Many people will execute their press and have little to no movement out of their scapula, thus causing increased stress on tissues that shouldn’t need to encounter them.
3) Lack of External Rotation
One of the issues many clients face is the inability to rotate their humerus back. This is more than just the presence of too much internal rotation (such as with U.C.S.). The muscles responsible for external rotation of the shoulder are powerful muscles that also engage in the motions of the scapula. Lacking strength in these tissues can cause someone to become more internally rotated, but also makes it incredibly hard to achieve external rotation at the glenohumeral joint.
This matters for more than just mobility.
Popular exercises such as pull-ups require a person to own a certain amount of external rotation in order to execute the motion. So too does the overhead press. Lacking the ability to achieve optimal end range of E.R. makes both movements, and so many others, hard to accomplish.
It is important to understand that the exercises we use to improve external rotation put the humerus in a greater rotation than we would normally encounter in traditional lifting. But, this sort of work is necessary to strengthen and stimulate the muscles that create E.R. and maintain it in an isometric contraction (such as during a overhead press).
4) Weak Core and Poor Thoracic Extension
As stated earlier, the core and spine play a major role in whether the shoulders function optimally. A lot of lifters never develop optimal shoulder health because they create mobility by overextending their lumbar and thoracic spine to compensate. This is especially prevalent in ego lifters performing an overhead press with a massive amount of “layback”.
Lacking the ability to contract the anterior core and stabilize the lumbar spine makes it significantly harder for someone to master true thoracic extension. The ability to lift the ribs and extend the thoracic spine allows for better depression, retraction, and downward rotation of the scapula. These motions are direct opposites of the posture that many fall into as a result of upper cross syndrome or “desk posture”.
Strengthen the abdominal wall and muscles of the T-spine is imperative to optimizing shoulder function. Much like the foundation of a skyscraper must be firm and set underneath the construction, so too does our core and spine for our shoulders.
5) Weak Upper Back and Lack of Awareness
In a lot of cases, especially in individuals who do not regularly engage in an exercise plan, there is simply a lack of proprioception and strength in the muscles that control the scapula and glenohumeral joint. Often, there is nothing “wrong” with this population other than their lack of sensory awareness and force production capabilities.
Clients like this require more exposure to well-coached patterns and a progressively overloaded strength program that allows their muscles to adapt over time. It may be beneficial to use low intensity correctives to prime a specific pattern and create mobility in the joint prior to loading the muscles with traditional methods.
It is critical that we stop seeing all clients as wrecked when they are unable to perform a specific task. For many people, especially with something as obscure as the FMS, it is simply an unfamiliarity with their body and the demand you are placing upon them. Increase their exposure to well-coached exercise instead of trying to fix something that isn’t broken.
New Solutions
As we dive into the specific movements it is important for us to realize that these are just a few examples of great movements that can be used to strengthen and stabilize the shoulder joint. Some of these movements are common and others are painfully boring (in a sense that we aren’t shaking the Earth).
However, simplicity is often the fasted route to success.
A few of these movements are going to be outside the realm of normality for some coaches. Many traditional strength coaches would look at Animal Flow as a weird form of yoga and dancing, but it is that arena that brings the fascia into the fold. Other movements are simply manipulations of variables in the training arena, such as the angled press, that most people aren’t considering.
1) Dual Kneeling Band Pull Apart
https://www.youtube.com/watch?v=3rrHNDcVa9s
The band pull apart is nothing new.
However, adding in the kneeling position asks us to contract our core and our glutes – two major parts of our foundation. In doing so we can better extend our thoracic spine, which in turn allows for better retraction of the scapula.
2.1) The Full-House (2 Cables/3 Motions)
https://www.youtube.com/watch?v=COSRT7nPTPc
This multi-pattern movement asks for retraction of the scapula, then retraction into downward rotation and depression (with external rotation of the humerus). Lastly, the overhead press asks for elevation, upward rotation, and forces the external rotators to fire hard to prevent the arms from collapsing forward of the line of gravity.
This sort of movement is incredible for grooving the scapulohumeral rhythm, improving upper back strength, and increasing external rotation of the humerus. It is quite the challenge and needs to be done extra light. Five pounds was the resistance in the videos.
2.2) Second View
https://www.youtube.com/watch?v=Qt8ex9TL8GQ
3) External Rotated T, Y
https://www.youtube.com/watch?v=3Juj1iYiJFE
A simple variation of traditional T and Y – this a movement that can be used to improve retraction of the scapula while strengthening the external rotators. It forces the trainee to own their humeral position and originate movement from the glenohumeral joint while remaining set onto stable scapula.
This exercise also promotes additional thoracic extension.
4) Angled Press
https://www.youtube.com/watch?v=FVPsVXWXds0
Far too many people contraindicate the overhead push pattern when someone is dealing with shoulder dysfunction. If we were to listen to the FMS, no one who can’t get a two on the shoulder mobility exam should ever press overhead. Yet, tons of people can press pain-free without getting a two.
This exercise helps bridge the gap between overhead pressing and not. The slight angle (about 15 degrees) allows you to load up the deltoids a bit without creating a perfect opposition to gravity. The neutral grip, forward elbow, and emphasis on tempo allows us to focus on scapulohumeral rhythm. Use this as a primary exercise after preparing clients for their workouts. This will correct a lot of flaws so long as the movement remains pain free.
5) Supinated Pulldowns
https://www.youtube.com/watch?v=TbIy3pH0nlo
At first glance this looks like a standard, boring pulldown.
Yet, it is the dramatic emphasis on depression and elevation of the scapula that makes this one stand out. Far too many folks get on the pulldown and just start yanking on the bar to get their set done. The motion becomes about completion instead of optimization.
The supinated hand grip helps keep the humerus in a slightly more externally rotated position while also prevented much of the internal rotation that happens with heavy pronated pulldowns. The focus here is to emphasize absolute end ranges. Feel the scapula elevate while maintaining control and then drive them downwards into full depression at the bottom.
6) Simple Animal Flow (Beast Hold to Scorpion to Alternating Crab Reaches)
https://www.youtube.com/watch?v=x27wT-nxUkg
A lot of you will look at this and wonder – why in the heck am I going to do all that flailing? Yet, animal flow is an incredible discipline that emphasizes loading of a lot of our passive structures – the fascia, the connective tissue, the skeletal system. Strengthening these things is imperative to the absolute realization of healthy shoulders. Specifically, the external rotation of the humerus in set crab position is a great tool to have in your arsenal.
7) BONUS: New Way to do Chest Flyes
https://www.youtube.com/watch?v=hcRTVz4aWOE
Lastly, I want to share the new best way for you to execute chest flyes.
See, the chest flye is one of the most favorite exercises in bodybuilding culture. It causes a tremendous stretch of the pec fibers and can help the person doing them build the muscle they crave. Yet, there is a ridiculous amount of sheering force placed upon the shoulder joint when the dumbbells reach the bottom of a traditional flye.
So, instead of using dumbbells and pissing off your shoulders – integrate this band only variation. The key is to press out into the band for the entirety of the movement, thus keeping a high level of tension on the working muscles without stressing the shoulder joint against gravity. As you fatigue shorten the range and focus on the squeeze.
Putting It All Together
You can correct someone’s shoulders and move their fitness forward at the same time. Your job as a fitness professional is to drive your clients towards the results they want and the results they didn’t know they need. You can still use low intensity correctives in your programs, of course, but it is imperative to go forward understanding that they are simply a very small piece of a much larger puzzle. Your client, if they are to improve, must begin strengthening the muscles by training the appropriate patterns that address shoulder health.
Next: The Lower Back and Pelvis
In the next article we’ll explore the lumbar spine, pelvis, and anterior core and how we can better correct chronic low-level back pain, coach better hinge patterns, and improve our client’s ability to move with confidence.
My friend and colleague (and author of the brand spankin new book, Day By Day: The Personal Trainer’s Blueprint to Achieving Ultimate Success), Kevin Mullins, reached out to me recently and asked, “Tony, why don’t you wear pants when you coach can I write a series for your site that covers joint/segment-by-segment breakdown and how to train to improve those regions WITHOUT going too far down the corrective train?”
Kevin understands people don’t have 40 hours per week to train and he’s found a sweet spot with his clients that improves function, hacks away at pain and immobility, and delivers results.
And, he wants to share that shit with the world (<– my words, not his).
Today’s post sets the tone on the over-inundation of corrective exercise (something I wrote about recently HERE), and each week (or two) after that, he’ll discuss a part of the body – shoulders, mid & low-back, and ankles, knees, & hips – and smack everyone in the face™ with how to improve function in that area.
Every year seems to bring a new set of ideals into the world of fitness. On one hand it is exciting to see that there are constantly new ideas, concepts, and tactics being brought into play. Much like living in a city with a lot of construction going on – it’s a good sign when the economy can support growth. The fitness industry, like a budding metropolitan area, is on the upswing.
Demand couldn’t be higher for products in the health and wellness field – as the modern world continues to gain weight and lose function. Millions of people around the world are ready to spend their hard-earned money on anything that will be a solution. It doesn’t matter if the goal is to lose weight, build strength, improve athleticism, get out of pain, or simply recreate the dance battle from the end of Step Up 2 – there is a product out there for them.
Having “money-on-the-table” is key in commercial real estate; a contractor must be confident that someone can afford the building project that is being proposed. When a company, such as a wealthy investment firm, wants to build a high rise and can prove they have the capital, the flood gates open and the contractors start fighting each other for a seat at the table.
In fitness, the “money” is on the table and the eager fitness professionals out there know it.
Personal websites and social media profiles have made “internet-fame” possible for anyone with a camera, microphone, and a desire to make money and be heard. This sort of opportunity has brought forth a litany of incredible fitness professionals that we might not know of otherwise. Just as the music industry found Justin Bieber on YouTube, many great coaches have been found in blogs and videos.
(I know this because I’m one of them).
Yet, with all things that are good in this world there exists the potential for them to turn bad. In this instance the unflinching availability of fitness advice makes it easy for bad information to get out, poor ideas to propagate, and for biased, and unfortunately dense, coaches to steal the spotlight.
In 2018 that spotlight was on all things corrective exercise.
It seems like everyday brought a new way to mobilize this joint, stabilize that segment, and improve breathing capacity by .00002ml.
Coaches from the furthest reaches of physical therapy school began talking about the need to invest hours on mobility, stability, and corrective work each week. Products began flowing into the industry like candy out of torn bag of skittles. Before long everyone was tasting the proverbial rainbow with their favorite flavors in hand: foam rollers, lacrosse balls, Theraguns, foot straps, mini-bands, mobility towels, and specialized assessments derived from the ancient wisdom that powers the Iron Fist.
Note From Tony: ^^^ This show is not as good as Punisher, DareDevil, Jessica Jones, Luke Cage, or watching a dog take a shit in a yard for that matter.
It’s open season on corrective exercise in the fitness industry – a modern day gold rush of fitness equipment designed to drain your wallet and decorate your home with odd instruments of pain and pleasure.
What a glorious time it is…
Let’s Be Clear Though:
Developing one’s mobility – especially in troublesome joints such as the shoulders, thoracic spine, hips, and ankles is never a bad thing. Most people spend twelve hours a day sitting at desks, in cars, and on couches, all in poor posture that stresses their spine, weakens their bodies, and causes long-term health risks to take hold. Every person reading these words can benefit from working on their mobility, except for Kelly Starrett (if he’s reading this) since the guy is a Supple Leopard.
Improving your segmental stability is also important.
Many people struggle with maintaining tension in their core, their mid-back, and their hips and legs. This lack of tension correlates to weaknesses that cause posture to degrade over time. Lifting heavy gets harder too. Weak muscles and poor neural connections make force production elusive.
Specific corrective exercises have their place too.
We are all a little messed up.
Some people have whacky shoulders, while others experience low back pain. Runners often have achy knees and tightened fascia in their shins and ankles. Other folks are pretty jacked up head to toe. For any and all of these people there are certainly movements and therapies that can be done to improve their condition and inch them closer to optimal performance capacity.
But:
A personal trainer’s job is to accomplish these things while also moving the ball forward in terms of their client’s fitness level. Far too many coaches obsess over the missing ten degrees of mobility in someone’s scapular downward rotation and depression while ignoring the additional forty pounds hanging out in their midsection.
Other coaches refuse to load a client even a little until their form in a movement is beyond perfect.
Even then they’ll question whether the client can repeat the performance in future sessions and insist on three more workouts with just an unloaded barbell to make sure. Meanwhile, no sweat has been released and no forceful stimuli are placed against the body. The client might end up with the best looking back squat form in the world (with a forty-five-pound bar), but that is about it.
This sort of absolutism and obsession is not good for a client and not good for the fitness industry either. If a client’s issues are so severe that any sort of intensity causes a series of negative events in their kinetic chain, pain, or lingering discomfort, then they must be referred out to physical therapist, or whatever medical specialist could heal their ailing.
Again, on one hand it is awesome to see so many coaches taking their client’s joint health, core strength, breathing quality, and fascial integrity so seriously. It is much better than an undereducated jack-wagon haphazardly throwing intensity at people in hopes that it gets them in shape and they keep paying. Nothing is more disturbing than a coach who lets their client put themselves at risk of serious injury repetition-after-repetition and session-after-session.
Yet, the coach who spends forty minutes of a sixty-minute session on a variety of implements meant to “improve” a person’s health is still quite the foul. People are paying for the results they want while also experiencing the growth that they don’t know they need, and our job is to give it to them.
Our job is not to force our obsessions upon them while completely ignoring their goals and needs.
A great fitness professional is someone who understands that self-myofascial release and zero-intensity correctives are just tiny pieces of a much larger puzzle that they must solve.
This series of blogs aims to bridge the very gap that has formed in the industry over the last few years. Over the next three installments you’ll find very specific methods of integrating new and better corrective strategies in each of the important joint segments of the body.
Those segments are:
Scapulothoracic Region and Glenohumeral Joint (Shoulder/Shoulder Blades and T-Spine)
T-Spine, L-Spine, and Pelvis
Ankle to Knee and Knee to Hip
Each one will work to answer the following question:
“How do we as a profession properly apply all of the information and modalities that emerge while still honoring the primary function of our profession (deliver a fitness stimuli to create a fitness result)?”
Our job as fitness professionals is to deliver the results our clients want while also giving them what they don’t know they need. As stated earlier, this sort of juggling act is hard to accomplish in a world where some trainers are exchanging thrash for cash and others are acting as extensions of physical therapy (when they aren’t qualified to do so).
The fact that you are already here on Tony’s site demonstrates that you aren’t like a lot of the “noise” of the industry. You realize that heavy things need moving, that the body needs a little oil and grease every now and again, and that hard work is the only pathway to really cool results. The fact that you clicked on this article demonstrates that you are looking to improve your methods, clean up your practices, and deliver better results for your clients.
Some of you might be shaking your head and clenching your fist right now.
You are thinking, “who is this Kevin Mullins guy and why in the hell does he think he can tell me that corrective exercises are a waste of time.” If that is you, then I want to say that I’m sorry if that is how you are reading this – it certainly isn’t my intention.
My goal is to help, in whatever way I can, move the ball forward so that we can continue to deliver better results to our clients in a variety of ways. In my opinion, absolutism is never good practice. It doesn’t work in politics and it doesn’t work in fitness. We must be willing to accept that there is always a better way to do something or else innovation will cease to exist.
Others of you might be wondering where I’m going with this piece.
Heck, you might even be a little irritated that you’ve read this much and didn’t access the secrets to hacking the body and winning the lottery every day. I apologize to you too. I just wanted to set the table for the first of three mega articles that are going to dive into the anatomy, physiology, and practical exercise and program design.
And so, I conclude our teaser with this important quote that I’ve taught every client, and fellow trainer, since I concocted it a few years back:
“It is important to always remember that strength causes stability – stability allows for mobility – and mobility improves the speed and accuracy for which strength can be executed.”
See you next time for a deep dive into the scapulothoracic region, the glenohumeral joint, and the core.
About the Author
Kevin Mullins, CSCS, is a personal trainer and group exercise instructor at Equinox Sports Club in Washington D.C.
Kevin utilizes a listen first, coach second strategy to ensure his clients, and programs, are exceptional…and not his ego.
When he isn’t training clients or writing content Kevin can be found deadlifting, Bicep curling, or finding new, corny ways to emphasize squeezing the glutes. Kevin maintains his own personal site HERE.
When it comes to neck pain, as a strength coach, I (generally) don’t touch that with a ten-foot pole. It’s case dependent of course, but more often than not, if someone I’m working with walks in with a some significant discomfort in their neck I 1) start hyperventilating into a paper bag and 2) immediately refer out to a someone who has more diagnostic and manual therapy skills.
This is not to say, however, that there aren’t any avenues to take if you’re a personal trainer or strength coach. It’s not like you can’t do anything. In today’s guest post physical therapist, Dr. Michael Infantino, goes into great detail on some things to consider if you ever find yourself in this predicament.
The Gym Is a Pain In My Neck: Two Movements To Cure Them All
Are you struggling with neck pain?
Does the gym make it worse?
Do you find yourself looking at a lot of informative websites for ways to resolve these issues, but wish it were compactly put in one place?
Does this sound like an infomercial?
Well it’s not!
But for just $29/month you can… just kidding.
This article is here to solve all of those problems. Neck pain is often blamed on poor form when exercising. This is absolutely true. Unfortunately this does not answer a crucial question, “why?” Discovering WHY your form is poor is the goal. On top of that, people often fail to recognize other human errors that are contributing to their symptoms. We will provide a guide for figuring out why you have neck pain and how to resolve it.
In most cases, pain attributed to the gym can be tied to the following:
Limitations in the necessary mobility to perform a movement
Limitations in the skill needed to perform a movement
Limitations in the capacity to perform a movement (Strength and Endurance)
Human error [Electrolyte and Fluid balance, Self-Care, Rest, Sleep, Breathing, Posture, Medication and Fear.]
Limitations in MOBILITY: 2 movements to cure them all!?
Limitations in your ability to put yourself in optimal positions during almost any upper body movement are a result of two movement limitations.
Limitations in these positions can lead to a host of different complaints. For the sake of time we are going to pick on NECK PAIN. If you are struggling with one exercise you are likely struggling with another, you just might not realize it.
Position #1: Shoulder Extension Test
Movements: Push Up, Pull Up, Row, Dip, Pull Up (top), Jump Rope, Punching someone in the nose because they have one of those weird miniature poodle mixes.
Attempt to perform the ^^THIS^^ motion
Instructions: Keep the neck retracted while extending the shoulders just beyond the trunk without the following:
Increased forward head position
Forward shoulder translation
Shoulder shrug
If you are unable to replicate the picture above you likely have a MOBILITY problem.
If you can’t perform this motion when you aren’t under load, you will definitely struggle when you are. Especially with repeated repetitions and the addition of weight.
Target Areas for Treatment
Soft Tissue Mobility
Pecs
Serratus Anterior
Upper Traps
Stretches and Joint Mobilization
Chin Retraction
Thoracic Extension (arms overhead)
Open Book Stretch
After working these bad boys out I want you to RE-CHECK the test position.
Is it better?
If not, you need to keep working on it.
Assuming you now have the necessary MOBILITY to perform this motion, we need to make sure you have the required SKILL with the particular movement you are interested in.
Skill: the necessary strength, stability and coordination to perform the most basic form of a loaded movement (pull up, push up, dip, row, etc.).
Are you able to maintain a good position in the:
Bottom of your push up
Row
Top of your pull up
Bottom of your dip
Jump roping
As you load the arm for a hay maker!
We aren’t as complex as you might think. Many of our daily activities are broken into a few movement patterns.
Follow this sequence:
Create the mobility necessary to perform the pattern in its most basic form. (In this case, Position #1 and #2).
Ensure you have the skill needed to perform your desired movement (Push Up, Pull Up, etc.)
Build capacity with that movement (Endurance and Strength).
If you don’t have the skill to perform a specific exercise or movement, you need to practice. Look at the above definition of skill to make that judgement. If you don’t have the baseline strength to perform one good push up, pull up, dip or row, see below for regressions that will allow you to maintain good form as you work your way back to mastering these moves.
Here are some ideas:
Push Up: Inclined position (Ex. against weight bench or counter), knee push ups
Pull Up: Assisted with a band, inverted row
Dip: Assisted with a band, bench dip
Row: Kind of an outlier since this move typically doesn’t require body weight. Use a weight that allows good form. TRX Row and inverted row are body weight options. Adjust the angle of your body to reduce the difficulty.
The goal here is to demonstrate the ability to maintain proper form throughout each movement with a regression that is appropriate for you.
Joe Muscles next to you may need to take 50 lbs. off his 200 lb. weighted belt during his pull-ups to maintain good form. You may need to work on getting one pull up with good form without any extra weight.
Most of us have one or two good pull ups in our bag of tricks to whip out for an “impromptu” Instagram post. Preventing injury is going to require you to build the strength and endurance to exceed Instagram’s one-minute time cap. DAMN you Instagram!
Adding repetitions and weight to the regression will help you work your way back to a standard pull up, row, dip, push up, etc.
I can’t emphasize this point enough.
We all have high expectations of ourselves. Neck pain after 10 reps is not necessarily a “push up” problem. It may be the fact that you did three other exercises before push ups that started to fatigue the neck. The push up was the breaking point. You need to have a realistic expectation of your current ability, or capacity.
Position #2: Overhead Test
Movements: Overhead Press, Pull Up (bottom position), Snatch
Instructions: Lie on your back with knees bent. Tuck chin (neck flat to ground) with arms flat to the ground in the start of a press position. Press arms overhead by sliding arms along the ground.
Common Faults:
One or both arms come off the floor at any point in time.
Compensatory forward head or extended neck position to keep arms on floor
Compensatory spine arch to keep arms on the floor
Assuming you repeatedly tried to replicate this position without success, once again we have a MOBILITY PROBLEM.
Target Areas for Treatment
Soft Tissue Mobility
Pecs
Lats
Rhomboids
Stretches and Joint Mobilization
Chin Retraction
T-Spine Drop In (or T Spine Extension)
Open Book Stretch (Add: External Rotation at Shoulder)
1st Rib and Scalene mobility
After finding the weak link, it is time to RE-CHECK. If it looks better, great let’s move on. Similar to Position #1, assuming you now have the pre-requisite MOBILITY to perform this motion we need to make sure you have the SKILL necessary.
*If you are having trouble improving your mobility or resolving pain, seek the advice of a qualified medical provider or fitness professional.
Can you maintain the same control and form during your overhead press, snatch, hang position of your pull up (or any variation- kipping pull up, toes to bar)? If not, we need to REGRESS the move. Unlike the shoulder extension position, many of the overhead exercises can be regressed by reducing the weight or working on single arm presses instead of two arms. Other regressions include:
Regressions:
Overhead press: Landmines (Tony goes into more depth in this article).
Snatch: Cleans, Single arm overhead kettlebell squat, single arm overhead lunge
Pull up (bottom): use a resistance band for support, inverted row
Human Error
Now that you have mastered Position #1 and #2, it is time to make sure that you are limiting HUMAN ERROR.
I think everyone should have someone in their life that serves as an extra pair of eyes. Even the best fitness trainers and medical providers in the world have a hard time being objective toward different areas of their own life. Barbers don’t cut their own hair, right? Not positive about that one. Either way, you can’t go wrong with some quality feedback!
Most of us are quick to blame the boulders in our life when it comes to pain, but we overlook the pebbles.
With pain we can’t overlook the pebbles.
The pebbles are diet, water intake, sleep, and self-care habits.
Patients usually tell me that they are doing “better than most” or that they are “pretty good” about optimizing these areas of their life. It isn’t until their spouse shows up to the appointment that we get the whole truth.
I love it!
Proper Fluid and Electrolyte Balance
Paying attention to what you consume pre and post workout is important. Proper fluids and electrolyte intake prior to exercise can help delay muscle fatigue and cramping.
Many people can get by with less than optimal effort when it comes to this category. However, if you are having neck pain you need to give yourself the best chance at success.
“At least 4 hours before exercise, individuals should drink approximately 5-7 mL·kg−1 body weight (~2-3 mL·lb−1) of water or a sport beverage. This would allow enough time to optimize hydration status and for excretion of any excess fluid as urine” (Sawka, 2007).
This is not always possible, I understand. Do your best. Some is better than none.
Warm Up
Proper warm up is also important.
Engaging in a warm up that gradually increases heart rate and muscle flexibility is a great way to prime the muscles. Dramatic increases in blood pressure and heart rate can lead to less than optimal muscle performance and increased risk of exertion headache during your workout.
Your warm up should be focused on getting the heart rate up; along with preparing the body for the movements you are going to perform during your workout (squat, push up, deadlift, clean, etc.).
Taking the time to stretch and do some soft tissue work after exercise will help reduce muscle soreness in the days following your workout (Gregory, 2015).
Leaving your body more prepared for the next workout. It is a great way to improve muscle extensibility and eliminate trigger points that aren’t allowing your muscles to perform effectively (Lucas, 2004).
Adequate rest is also important for recovery.
Going hard every day and not getting adequate sleep does not allow your body to grow and repair itself. Neglecting proper recovery leads to a less than optimal immune system and central nervous system.
Sleep deficits can also lead to an increase in the intensity of pain and alterations in mood. This is some serious shiznit. Can’t express enough how important this category is. I am a huge fan of the “grind.” It just sounds cool. You aren’t meant to grind everyday though, so please take some time to recover.
Breathing and Posture
Proper breathing is something that is often overlooked, but may be contributing to neck pain.
Gritting it out is cool, I highly recommend it. It builds character.
However, regularly holding your breath or clinching of your teeth when exercising can lead to increased tension around the neck. This could end up resulting in tension headaches as well.
Many of us without realizing it spend most of our day performing shallow breaths. We often over utilize the neck musculature. Shallow breathing into the chest can increase tension in these muscles and even increase feelings of anxiety.
It is recommended that people learn how to perform relaxed diaphragmatic breathing to reduce tension in the neck muscles. Staying in sustained postures throughout the day can also be contributing to your neck pain.
Many studies continue to show that sustained postures throughout the day (typically with office workers), especially with a forward head position, can increase neck pain and headaches (Ariëns, 2001).
Symptoms are also more common in people that hate their job.
Really off topic, but it is true …
Consider how stress in your life (emotional or physical) is amplifying your feelings of pain. Emotional pain and physical pain are HEAVILY connected. Check out this video by Tony to learn a little more about proper breathing strategies.
The Advil Fix
This may not seem to fit with the other categories.
Nonetheless, it is super important.
Side effects related to over the counter anti-inflammatory use are becoming common knowledge. Every now and then I run into someone that isn’t aware of the potential risks of regular use.
Popping over the counter anti-inflammatories (i.e. advil) before or after your workouts IS NOT recommended.
It’s like sweeping the dirt under the rug.
“The most common side effect from all NSAIDs is damage to the gastrointestinal tract, which includes your esophagus, stomach, and small intestine. More than half of all bleeding ulcers are caused by NSAIDs, says gastroenterologist Byron Cryer, MD, a spokesperson for the American Gastroenterological Association.”
Fear
One of the reasons that I started RehabRenegade.com was to help share information like this with as many people as possible. Many of the complaints I get in clinic can be fixed SUPER QUICK. Having a basic understanding of how to care for yourself and knowledge of the body can remove the “threat” of pain.
Red flags (serious pathology) represent less than 2% of the cases that are seen in a clinical setting (Medbridge, Chad Cook: Cervical Examination).
The Internet can be a blessing and a curse.
It can either lead you down the right road or scare the living crap out of you. We all know that any injury or illness is usually presumed to be cancer after a late night search on WebMD. Here are some discussions and advice I found on the inter-web related to neck pain in the gym.
Great intentions, but poor advice.
We tend to blame everything on a “pulled muscle,” whatever that means.
Rest?
What year is it?
We stopped recommending straight rest in like 1902.
By all means, take time off from the gym.
This doesn’t give you free rain to lie in bed all day watching re-runs of Game of Thrones.
It’s true… you may have over done it. Your muscles were overworked. Likely leading to a nice amount of local inflammation and some trigger points. The more constructive advice would be to perform some soft tissue work, light stretching and low intensity non-painful exercise to keep that area mobile.
Resorting to pain medication is not a healthy option. Last but not least, mentioning damaged discs and compressed nerves never makes someone feel at ease. Trauma to the neck may be a reason for disc injury. Overdoing your push ups and pull ups is NOT.
Fun Fact: The prevalence of disk degeneration in asymptomatic (without symptoms) individuals increased from “37% of 20-year-old individuals to 96% of 80-year-old individuals. Disk bulge prevalence increased from 30% of those 20 years of age to 84% of those 80 years of age” (Brinjikji, 2015).
Positive findings on MRI are common in people without pain. Don’t get too caught up in images and diagnoses. Do the things we know are healthy. If you hit the gym hard this morning and then followed that up with a CROISSAN’WICH from Burger King, and a cigarette at lunch we have bigger fish to fry.
First and foremost, muscle and joint strain at the neck commonly refers pain to the head. We call this a cervicogenic headache. Rest assured that it is very rare that you have a more serious pathology requiring immediate medical attention. Give the tips in this post a shot, if it doesn’t help by all means see a medical professional. The worst thing you can do is show up to your medical provider without attempting to improve your flexibility, tweak your form or get adequate rest.
If I had a dollar for every time a therapist told someone they had the tightest (fill in the blank) they have ever seen I would be a little better off.
If this poor girl wasn’t worried enough… Now she has the tightest back he has ever seen… really?
As providers we need to be very careful with our words. It is really easy for us to turn neck pain into chronic neck pain.
It is called an iatrogenic vortex.
When people get tied up in the medical system too long they often see symptoms worsen or develop other unexplained diagnoses.
Overview
In most cases, pain attributed to the gym can be tied to the following:
Limitations in the necessary mobility to perform a movement
Limitations in the Skill needed to perform a movement
Limitations in the Capacity to perform a movement (Strength and Endurance)
Human Error [Electrolyte and fluid balance, Self-Care, Rest, Sleep, Breathing, Posture, Medication and Fear]
You could be one small modification away from eliminating your neck pain.
The big takeaway here is to make sure you have the ability to perform various exercises with good skill.
From there, you need the knowledge and self-awareness to know when you have exceeded you capacity.
You also need to look at the big picture to ensure that you are checking the boxes when it comes to living a healthy life. If you are someone that often finds yourself worried or anxious when injury sets in please take a step back and look at the big picture. Use this article to see where your gaps are. If you still can’t get relief please see a medical provider. Nothing makes medical providers happier than working with patients who demonstrate a willingness to learn and grow.
About the Author
Dr. Michael Infantino is a physical therapist. He works with active military members in the DMV region. You can find more articles by Michael at RehabRenegade.com.
References
Ariëns GAM, Bongers PM, Douwes M, et al
Are neck flexion, neck rotation, and sitting at work risk factors for neck pain? Results of a prospective cohort study. Occupational and Environmental Medicine 2001;58:200-207.
Brinjikji, W., Luetmer, P. H., Comstock, B., Bresnahan, B. W., Chen, L. E., Deyo, R. A.,Jarvik, J. G. (2015). Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. AJNR. American Journal of Neuroradiology, 36(4), 811–816. http://doi.org/10.3174/ajnr.A4173
Gregory E. P. Pearcey, David J. Bradbury-Squires, Jon-Erik Kawamoto, Eric J. Drinkwater, David G. Behm, and Duane C. Button (2015) Foam Rolling for Delayed-Onset Muscle Soreness and Recovery of Dynamic Performance Measures. Journal of Athletic Training: January 2015, Vol. 50, No. 1, pp. 5-13.
Lucas KR, Polus BI, Rich PS. Latent myofascial trigger points: their effects on muscle activation and movement efficiency. J Bodyw Mov Ther. 2004;8:160-166
Sawka MN, Burke LM, Eichner ER, Maughan RJ, Montain SJ, Stachenfeld NS. American College of Sports Medicine position stand. Exercise and fluid replacement. Med Sci Sports Exerc. 2007;39:377-90.



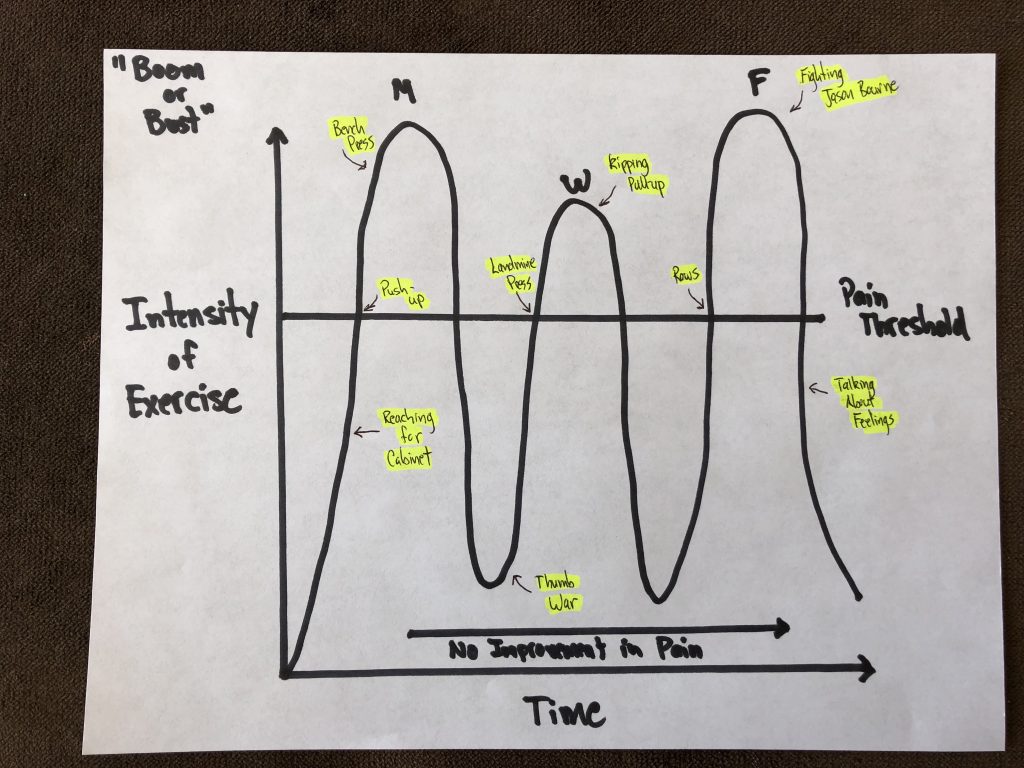
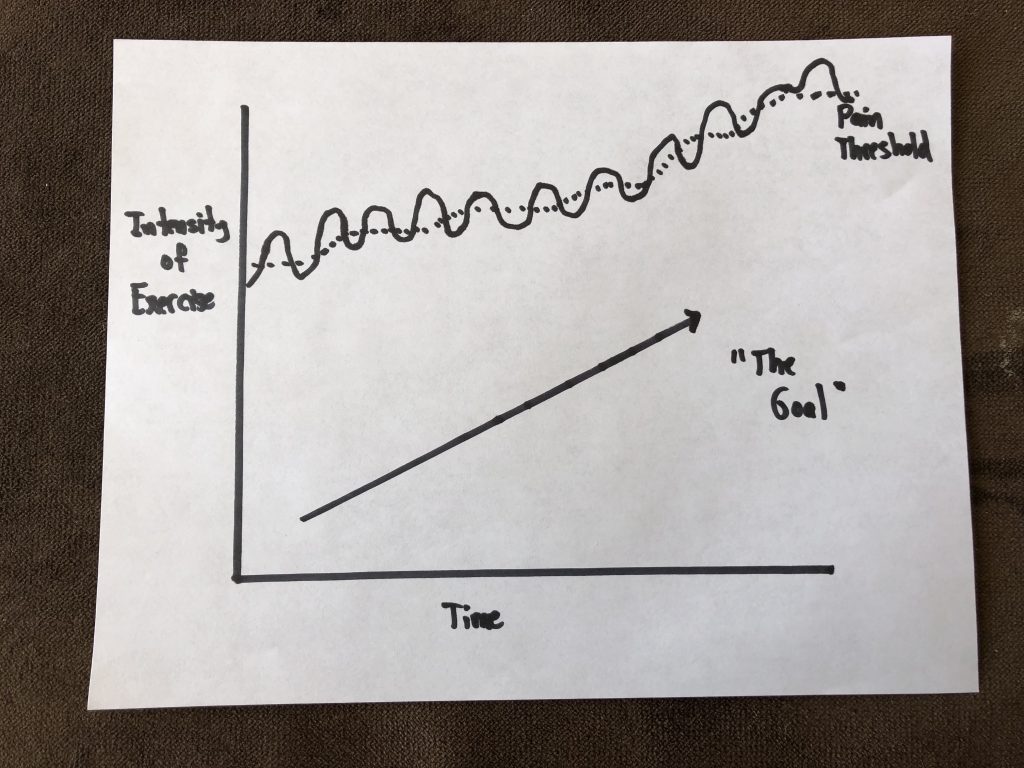









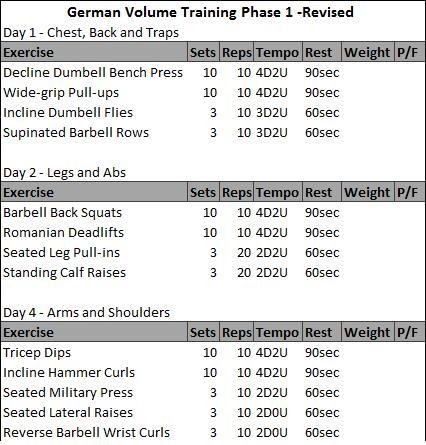











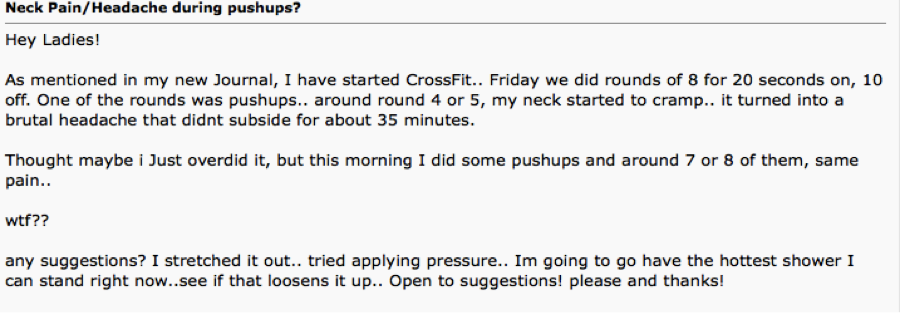
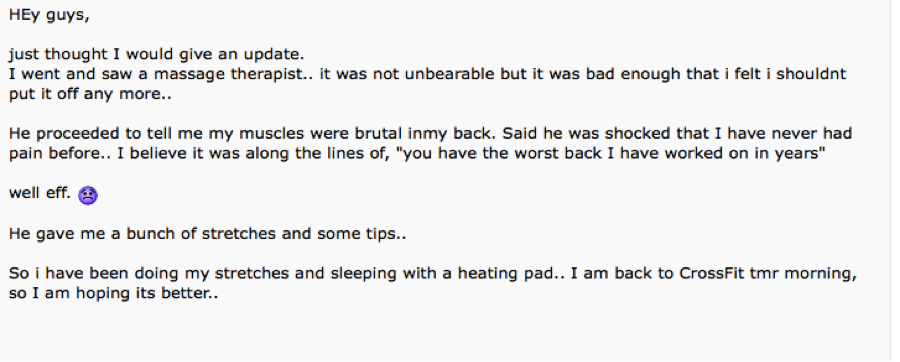
 Dr. Michael Infantino is a physical therapist. He works with active military members in the DMV region. You can find more articles by Michael at
Dr. Michael Infantino is a physical therapist. He works with active military members in the DMV region. You can find more articles by Michael at 

