There’s a lot that needs to be taken into consideration when assessing a new client.
Their unique injury history (past and present), goal(s), training experience, time constraints, equipment availability, even their favorite 90’s tv teen drama (if it’s not Party of Five we can’t be friends)…
…all are taken into account and cross-pollinated with my educational background and experience to ascertain, to the best of my ability, what will be the best course of action to get said individual from Point A1to Point B2 this means becoming in the most time efficient and and safe manner possible.
The assessment, at least from my perspective, is an amalgamation of muscle testing, movement screens, table work, and good ol’ fashioned investigative work to see whether or not something shakes free or if any “red flags” exist.
But more importantly, the assessment is a splendid opportunity to set the tone, prove to someone that they’re not “broken,” and to help them find their TRAINABLE MENU.
In short, I often joke that my assessment can be described as follows:
“Can the person standing in front of me do stuff?”
There’s only so much muscle testing, table work, looking at range of motion, and “hmmm’ing” and “ahhhh’ing” any one individual can tolerate before (s)he wants to jump through a pane glass window.
To that end, I prefer to make my assessments more palatable by getting the person standing/sitting in front of me more involved in the process and providing the “facade” (for lack of a better term) that they’re being taken through a pseudo training session.
By having him or her MOVE during their assessment I accomplish a few things:
1) I don’t come across as a creepoid by just staring at them for 60 minutes and stroking my beard (even though I don’t have one).
2) I get waaaaaaay more information in terms of movement ability, compensation patterns (if any) that exist, and whether or not certain positions (or loads) exacerbate their symptoms.
Active vs. Passive Assessment
One simple way to do all the above is to differentiate between one’s ability to actively perform a specific movement pattern and to passively do it.
My colleague, Luke Worthington, who’s my co-presenter in the Strategic Strength Workshop, states things very succinctly:
“What can THEY do?” = Active Assessment
“What can I do FOR them?” = Passive assessment.
Lets take the squat as an example.
When you watch someone perform a standard bodyweight (or loaded) squat you’re bound to see a bevy of things go awry.
Don’t get me wrong, it’s not always a shit show.
Every so often I’ll work with someone for the first time, they’ll demonstrate a well executed squat, and I’ll break down crying like the first time I watched the series finale of Andor.
However, if I’m being honest, this doesn’t happen often.3
Generally speaking there’s always something weird or wonky or twingey whenever I watch someone squat
No one is perfect.
But to that point, I think it’s imperative to differentiate between someone’s ACTIVE ability to do something and their PASSIVE ability to do it.
Watch someone squat and it’s likely you’ll see any one of the following (if not a combination):
Knee valgus
Excessive rounding of the spine
Excessive pronation of the feet
Loss of balance
A perceived lack of depth (<— which is arbitrary, but if there’s a lot of “effort” to get to a certain depth or it’s just really, really shallow, then that is important to note).
And when we do see any of the above we have a nasty habit of assuming that said individual is dysfunctional, and subsequently end up over corrective exercising them to death.
Fast forward three months (and a cornucopia of hip mobility and ankle dorsiflexion drills) and there’s been little, if any, improvement.
But don’t stop there; especially if you find they’re having trouble with it.
You should also test them PASSIVELY.
Oftentimes, when you add this extra layer of assessment, in a way that’s less aggressive and provides a bit more stability to the system – FYI: HERE‘s another way to do it in a quadruped position – you’ll find that they CAN do what you’re asking them to do.
Why Is This Important?
In the video above I’m taking my training partner, Justin, through a basic (passive) hip scour/hip flexion screen. If he were a client this would follow an active squat assessment.
I’d want to see if his ACTIVE movement (he’s doing the work) matched his PASSIVE (I’m doing the work). From there I’d want to compare the gap that exists between the two.
I want that gap to be as narrow as possible.
If his active squat was poor yet I re-assessed passively and saw an improvement – I.e., that he could, indeed, access more ROM – then I can surmise with a high degree of certainty that he doesn’t have a micro-penis he is likely not dealing with something more nefarious, like a bony block or musculature issue.
In this scenario I can do my job as a coach.
I can implement the appropriate “correctives” and/or exercise progressions/regressions to help him learn to squat.
His body showed me he can do it passively, so I need to show it how to do it actively.
If, however, there was no improvement when testing him passively, then:
It’s not my job.
1) I’d still work within my scope and train him within the ROM that’s pain free and that he can control.
2) However, I’d also refer out for more diagnostic testing or manual therapy to compliment his iron work.
Take Home Points
The assessment shouldn’t be used as a tool to point out every…single…dysfunction someone has.
Besides, what presents as “dysfunctional” actively may just be the body turning on the emergency brakes.
Also look at PASSIVE movement.
Try to narrow the gap between active ROM and passive.
If more ROM is present passively, then do what you do best…coach!
If ROM is poor (or pain exists) actively AND passively, you may want to consider referring out.
I don’t know, it could just be me, but Groutfits make my butt look amazing.
I often speak on the importance of the test/re-test concept with regards to assessment.
It’s nothing fancy or elaborate.
You test something – whether it be range of motion or maybe a strength discrepancy – implement a “corrective” modality if something’s deemed out of whack, and then re-rest that shit to see if it worked.
The test/re-test approach helps set the tone for any future “corrective” strategies or programming considerations you’ll do as a coach or trainer.
In addition, and something I’d argue is equally as important, it also provides an added layer of value to the assessment.
If you’re able to demonstrate to someone a significant change or improvement in ROM or reduction in pain/discomfort by implementing a drill or two, and it’s something they’ve been struggling with despite countless interactions with other fitness professionals, what’s the likelihood they’ll bust out their checkbook or Bitcoin wallets (<—depending on their level of geekery)?
I suspect highly likely.
It demonstrates a perceived level of “mastery” and knowledge-base towards the assesser (you) and, in a roundabout, reverse psychology kind-of-way, delves into the “pain center” of the assessee (athlete/client).
In this example it can refer to literal pain such as a banged up shoulder, knee, or lower back. But it can also speak to pain in the figurative sense too. Someone who’s frustrated and “had it up to here!” that they can’t lose weight, or maybe an athlete who was cut from their high-school team would have a degree of “pain” that would incentivize them to take action.
Show someone success or a clear path of action, however little, and they’re putty in your hands.
Of course this assumes you’re not some shady shyster who tries to up-sell the benefits of some super-secret concurrent, 47-week, Eastern-Bloc training program you copied from Muscle & Fitness or, I don’t know, organic raspberry ketones laced with mermaid placenta.
People who promote and use smoke-and-mirror tactics are the worst.
But lets get back to the topic at hand.
Test/Re-Test
One of the main screens I use with my athletes and clients is their ability to lift or elevate their arms above their heads.
Shoulder flexion is important for everyone, not just overhead athletes and CrossFitters.
If someone lacks shoulder flexion, and they’re an athlete, it’s going to affect their performance. A baseball pitcher may be “stuck” in gross shoulder depression, which in turn will have ramifications on scapular positioning and kinematics, which in turn will result in faulty mechanics and compensatory issues up and down the kinetic chain.
Conversely, regular ol’ Hank from accounting, who likes to hit the gym hard after work, if he lacks shoulder flexion, he too could have numerous issues arise ranging from shoulder and elbow pain to lower back shenanigans.
Shoulder flexion – and the ability to do it – is a big deal in my opinion. And it’s a screen that should be a high-priority in any fitness professionals assessment protocol.
So lets say I’m working with someone who lacks shoulder flexion. I test it both actively (standing, picture above) and passively (on a training table).
I surmise that it’s limited and that it may be feeding into why a particular person’s shoulder has been bothering him or her.
I can use the test/re-test approach to see if I can nudge an improvement.
Now, as I’ve learned from many people much smarter than myself – Mike Reinold, Sue Falsone, Dr. Evan Osar, Dr. Stuart McGill, Papa Smurf, etc – you shouldn’t rely on any ONE screen/corrective.
Everyone is different, and what works for one person might not even scratch the surface for another.
With regards to addressing (lack of) shoulder flexion5, there are a handful of “go to” strategies I like to use.
And then it’s just a matter of seeing which one sticks.
1) Encouraging a Better Position
In order to elevate the humerus (arm) above your head, the scapulae (shoulder blade) needs to do three things:
Upwardly rotate
Posteriorly tilt
Protract
The ability to do so is vastly correlated with the thorax. Those who are super kyphotic (ultra rounded upper back) will have a hard time elevating their arms overhead. Often, the simple “fix” here is to foam roll the upper back and work on more t-spine extension and you’ll almost always see an improvement.
Bench T-Spine Extension
Side Lying Windmill
But what about the opposite? Those who are stuck in more “gross” extension and downward rotation?
I.e., the bulk of athletes and meatheads.
Here the shoulder blades can be seemingly “glued” down.
In that case some positional breathing drills to “un-glue” the shoulder blades (and to encourage more 3D or 360 degree expansion of the ribcage/thorax) would be highly advantageous.
All 4s Belly-Breathing
It’s amazing what a few minutes of this drill can do with improving shoulder flexion ROM, without having to yank or pull or “smash” anything.
2) Allow the Shoulder Blades to Move
Some people simply don’t know how to allow their shoulder blades to move. A prime example is this past weekend.
An attendee who’s a personal trainer – but also competes in figure – mentioned how her shoulders (especially her left) had been bothering her for eons, and she couldn’t figure out why.
We had her perform this drill.
1-Arm Quadruped Protraction
In reality, both protraction and retraction are occurring, but many people have a hard time with the former.
The idea here is to learn to gain movement from the shoulder blade itself and not via the t-spine.
Here’s another angle (because, triceps):
https://www.youtube.com/watch?v=eyNFNxqFlSc
After a few “passes” with this drill, she saw an immediate improvement in her ROM. What’s more, the following day when she showed up for Day #2, the first thing out of her mouth was “my shoulder feels amazing today.”
That’s a win.
3) Pin and Go
Another route to take is to have the person foam roll their lats. Not many people do this, and there’s a reason why: It’s un-pleasant.
I’ll have the person spend a good 30 seconds or so on each side and then have them stand up and perform a simple SMR drill using a lacrosse ball against a wall.
They’ll “pin” the teres minor down (basically, find the tender spot behind their shoulder and hold it there) and then work into upward rotation.
https://www.youtube.com/watch?v=9OiGt_O1FvY
Another five or so passes here, and I’ll re-test.
Many times I’ll see a marked improvement in their shoulder flexion.
Caveat
NONE of this is to insinuate that anything mentioned above will work for everyone. The idea is to understand that it’s important to “test” a number of modalities and then re-test to see if you find an improvement.
If you do, you’re likely barking up the right tree which will make your corrective approach and subsequent strength training more successful.
The topic of low back pain (LBP) – how to assess it, diagnose it, and how to treat it – can be a controversial one. I italicized the word “can” because I don’t feel it’s all that controversial.
Cauliflower as an option for pizza crust or Zach being chosen as the bachelor on the current season of The Bachelor (when it’s 100% clear that a ham sandwich has more charisma) = controversial.
Simple stuff to consider to help with one’s LBP = not so much.
The topic of low back pain and how to address it is controversial because there’s no one clear approach or answer to solve it.
(And if the last 3+ years of this pandemic dumpster fire has taught us anything it’s that we looooooove to argue over what’s best and what works).
SPOILER ALERT: Everything and nothing causes LBP.
Have ten different doctors or physical therapists work with the same patient and it’s likely you’ll get ten different opinions as to what the root cause is and what tactics need to be implemented to resolve it.
One person says it’s due to delayed firing of the Transverse Abdominus (TA), while someone else states it’s due to someone’s less than great posture or tight hamstrings.
For the record, all are weak excuses at best.
The culprit can rarely be attributed to any ONE thing.
But it’s amazing how often “tight hamstrings” is the fall guy.
Low back pain? Tight hamstrings.
Knee hurts? Tight hamstrings.
Have Type II Diabetes? Tight hamstrings.
Brown patches on your front lawn? Hamstrings.
It’s uncanny.
I mean, I could just as easily sit here and say in worse case scenarios LBP results from drinking too much coffee. I have zero evidence to back that up, but whatever.
…neither do most of the other “culprits” people tend to use as scapegoats.
So, why not coffee?
Or Care Bears for that matter, those sadistic fucks.
What works for one person, may exacerbate symptoms for someone else. And as my good friend, Dr. John Rusin notes:
“Fact of the matter is: there is NO one right way. it’s a big mistake to lump all LBP into the same category and even a bigger mistake to assume all of it presents the same or should be treated the same.”
There’s no way for me to write a thorough blog post on such a loaded topic; especially one that will make everyone happy.
It’s impossible.
I have better odds at surviving a cage match with an Uruk-hai.
Part of me feels like the proper response to the question “what causes low back pain and what’s the best way to address it?” is this:
Most people reading aren’t clinicians or physical therapists. There’s very little (if any) diagnosing going on in the hands of a personal trainer or strength coach. And, truth be told, if you are a personal trainer or strength coach and you are diagnosing, YOU……NEED…….TO…….STOP.
Just stop.
It’s imperative to defer to your network of more qualified (and vetted) fitness/health professionals whom you trust to do that.
However, it’s important to also consider we (as in personal trainers and strength coaches) are often the “first line of entry” into the medical model. We’re the first to recognize faulty movement patterns, weakness, imbalances, and bear the brunt of questioning from our clients and athletes when they come to us with low back pain.
There’s quite a bit we can do to help people.
What follows is a brief look into my mind and what has worked for me in the past with regards to LBP; a Cliff Notes “big rock” brain dump if you will.
Sorry if I offended anyone who likes Care Bears.
1) Rest Is Lame
My #1 pet peeve (and many agree with me) is that “rest” is the worst piece of advice ever.
“Go stick your finger in that electrical socket over there” would be better.
This isn’t to say there aren’t extenuating circumstances where taking a chill pill is absolutely the right choice; sometimes we do need to back off and allow the body a window of time to heal or reduce pain/swelling/symptoms.
That said, I think it’s lame when a medical professional tells someone to “rest,” or worse, informs them that they’ll need to learn to “live with low back pain.”
It’s a defeatist attitude and will spell game over for many people. Before you know it they’re living on a foam roller and thinking about a “neutral spine” while washing their hands.
(NOTE: I am not anti-teaching neutral spine to people. It’s a lovely starting point for most people, but at some stage people need to learn to move in (and out) of precarious positions…because that’s life).
A common theme reverberated in the S&C community is to say “strength is corrective.” I wholeheartedly agree with this sentiment. In fact, why the hell has this not been made into a t-shirt yet?
However, I think a slightly better moniker may be to say:
“Movement is corrective.“
We can use movement (and yes, strength) to help people get out of pain. Rest has its time and place, but I find stagnation to be more of a problem.
The body is meant to move and is wonderfully adaptive. And that’s the thing: adaptation and forcing the body to react to (appropriate levels of) change and stress is paramount to long-term success with LBP.
Sitting on a couch watching Divorce Court in the middle of the day isn’t going to help.
2) Move, But Move Well
I was watching Optimizing Movement with Mike Reinold recently and he noted there are three key elements to movement and why someone may not do it well:
Structural Issues
Coaching/Technique
Programming
It’s important to understand that, in this case, everyone is a unique snowflake.
Structure: Anatomically speaking there is huge variance amongst the population. Hip structure, for example, can have a large effect on someone’s ability to squat to a certain depth or get into certain positions. Likewise, who’s to say the hips are always the culprit? Even upper extremity considerations – like one’s ability to bring their arms overhead (lack of shoulder flexion) – can have dire consequences on back health.
The body likes to use the path of least resistance (also the most efficient) to accomplish any task. However in this case, “most efficient” doesn’t mean best. As Reinold notes:
“Efficient in this case refers to energy, not movement.”
Lack of shoulder flexion will often lead to compensation via more extension through the lumbar spine. It’s efficient movement, but it’s not better movement.
Coaching/Technique: I’m a firm believer that everyone should deadlift (it’s a hip hinge, learning to dissociate hip movement from lumbar movement, doesn’t mean we have to load it), but I don’t feel everyone should do it from the floor or with a straight bar.
Cater the exercise to the lifter, not the lifter to the exercise.
More on this below.
Programming: If someone lacks hip flexion why have them conventional deadlift? If someone lacks shoulder flexion why have them perform overhead pressing or kipping pull-ups? Some of the onus is on YOU, dear fitness professional.
Find what actions hurt or exacerbate symptoms, and stop doing it.
I know I just blew your mind right there.
For example:
1. Client says “x” hurts, and then places their body into some pretzel like contortionist position that would make a Cirque du Soliel performer give them a high-five.
Me: “Um, stop doing that.”
2. But that could also mean addressing how they walk or how they sit in a chair. Someone with flexion-based back pain, will like to be in flexion, a lot.
Maybe taking them through a slump test will offer some pertinent info.
Have them start in a “good” position:
Then, have them purposely “slump” into excessive flexion:
Someone who is flexion intolerant – despite preferring to be in that position – will often say this causes pain.
Ding, ding, ding.
So, the “fix” is to coach them up and try to keep them out of excessive spinal flexion. Cueing them how to sit in their chair and to get up (wider base of support, brace abs, chest up), building spinal endurance (and strength) via planks, and having them hang out in more extension may be the right path to take.
3. On the opposite side of the spectrum is extension, which is often a problem in more athletic populations and in those occupations requiring more standing (ahem: personal trainers/coaches).
Here you might put them into extension and see what happens.
Much like people who are flexion intolerant “liking” flexion, those in excessive extension will like to live in extension.
This will likely hurt.
Finding their spinal neutral is key too.
Hammering spinal endurance/strength via planks (done well) still hits the nail on the head, as does nudging them towards exercises that emphasize posterior pelvic tilt (much of time cuing people NOT to excessively arch during their set up on squats and deadlifts), and even drills that promote spinal flexion…albeit unloaded.
Spinal flexion doesn’t always have to be avoided. In fact, it’s sometimes needed.
Either way, meticulous attention to detail on finding spinal neutral – or pain from ROM – is huge. Once that is addressed, and symptoms has subsided, we can then encourage them to marinate in more amplitude of movement, taking them OUT of spine neutral (cause, it’s gonna happen in everyday life) and use the weight-room to help strengthen those new ROMs.
But I digress.
4) Don’t Treat People Like a Patient
I know this will rub some people the wrong way, but I still use the deadlift for the bulk of people I work with you have LBP.
Nothing sounds so absurd to me than when I hear someone say how the deadlift is ruining everyone’s spines.
To recap:
Deadlift = hip hinge.
Hip Hinge = learning to dissociate hip movement from lumbar movement.
Mic drop.
Resiliency is key in my book. And not many movements make the body more resilient than the deadlift or any properly progressed hip hinge exercise catered to the individual’s goals, injury history, and ability level:
Assuming I have coached someone up enough to understand spinal neutral and they’re able to maintain it, why not poke the bear and challenge them?
A deadlift doesn’t always mean using a straight bar and pulling heavy from the floor until someone shit’s their spleen.
I can use a kettlebell and band to groove the movement:
I can also use a trap bar, which is a more user-friendly way of deadlifting as it allows those with mobility restrictions to get into a better position compared to a straight bar.
https://www.youtube.com/watch?v=p-sA3PG1kGY
Too, I have found great success with various other exercises:
Farmer and Suitcase carries
Shovel Holds
“Offset” loaded exercises like 1-arm DB presses or 1-arm rows, lunges or RDLs (where you hold ONE DB to the side and perform the exercise). It’s a great way to increase the challenge to the core musculature.
Or even outside-the-box exercises like Slideboard Miyagi’s
So long as we’re staying out of precarious positions or those positions which feed into the issue(s) at hand, we’re good.
Find a training effect with your clients/athletes.
Help them find their TRAINABLE MENU.
And That’s That
People have low back pain for a variety of reasons: They’re too tight, too loose, too weak, have poor kinesthetic awareness, or they’re left handed.
The umbrella theme to remember is that there is never ONE root cause or ONE definitive approach to address it across the board. However, that doesn’t mean there aren’t some “big rock” things to consider that will vastly improve your’s and their chances of success.
NOTE: There’s only a few more days to get my latest continuing education resource – Strategic Strength – at $50 off the regular price. Today’s post discusses one of the main topics covered in the course: Assessment.
Assessment.
People don’t like the feeling of being judged – especially by complete strangers.
However, when it comes to working with a coach or personal trainer for the first time, an “assessment” is pretty much standard procedure; a means to an end with regards to collecting data to better ascertain someone’s starting point.
In Short: An assessment guides the coach to help figure out the safest and most efficient path for a client to reach his or her’s goal(s).7
That being said…I feel many of us are approaching assessment the wrong way.
I am not writing this as an attack against assessment
Likewise I am also not here to say one way or the other how you should assess your clients.
You know your clients/athletes better than I do.
I don’t care if your assessment of choice is the Functional Movement Screen, the Selective Functional Movement Assessment, PRI (Postural Restoration Institute), DNS (Dynamic Neuromuscular Stabilization), FRC (Functional Range Conditioning), whatever institutions like NASM or ACE prefer, or, I don’t know, duck-duck-goose.
Everything has it’s strengths and weaknesses.
More to the point, I would think that as people progress through their careers they’d take it upon themselves to actively change their minds the more they learn and gain experience.
They’ll experiment more and eventually “cherry pick” from several modalities to best fit their philosophy and approach to training.
Ideally “assessment” should be a smorgasbord of reaches, rolls, carries, squats, hinges, toe touches, twists, presses, and bicep curls (<— only half kidding on that last one), among other things.
Here is Gray Cook’s definition of assessment (a good one, mind you):
“In the assessment you take your education background, your professional wisdom, the particular situation, the time constraints, other historical information like a medical history or previous problems…and put all that together. That’s an assessment.”
Pretty hard to disagree with that, right?
Here’s my lame attempt:
“Can the person sitting/standing in front of you do stuff?”
I’m not tossing darts at everyone, but I do find that the bulk of fitness professionals out there use the initial assessment as an opportunity to search every crevasse (not that crevasse, get your mind out of the gutter), nook & cranny, and area of the body for “dysfunction.”
Many use the assessment as an opportunity to demonstrate to someone how much of a walking ball of fail they are.
“Okay Mr. Jones here’s what we got: your hip flexors are tight, you have forward head posture, you lack frontal plane stability, you lack ample scapular upward rotation, your left big toe has zero dorsiflexion, you have weak glutes, you’re quad dominant, your shoulders are slightly internally rotated, you’re probably gluten intolerant, your wife is cheating on you, and I’m about 37% convinced you have cancer.
If you purchase a 24 pack you’ll save $13 per session. Whataya say?”
Some of the above may be relevant and stuff you should focus on as a trainer. I mean, I’m not going to sit here and belabor a coach for wanting to improve a client’s thoracic spine mobility.
However, if I were the person listening to some laundry list of things I suck at or need to improve on, I’d be like………
………..”fuck off.”
Be Careful of Being Told to “Fuck Off”
There’s much I can wax poetic on when it comes to the topic of assessment. My biggest pet-peeve, though, is when coaches/trainers place waaaaaaaaaay too much emphasis on someone’s resting/static posture.
Lets revisit the picture from above.
Many high-end gyms implement this advanced form of “postural assessment” as an up-sell to seduce more people into purchase training.
Said individual stands in front of a giant gridded screen and is then hooked up with a bunch of probes and what not that are placed at strategic locations around the body that bloop and bleep.
It’s reminiscent of one the most terrifying movies I have ever seen, Fire in the Sky.
Remember that one?
You know, that alien abduction movie from the early 90’s where the main character is relentlessly poked and prodded by a bunch of aliens on their spaceship?
It’s terrifying.
Anyway, I can’t help but be reminded of that movie whenever I see someone being told to stand in front of a grid so some trainer can scrutinize every inch of their posture in the hopes they’ll be hired to “fix” it.
Who says it needs to be fixed in the first place?
I’m reminded of a photograph shared by Fort Worth, TX based physical therapist, Dr. Jarod Hall a few years back which hammers home my point.
Here’s what he said/posted:
“I want everybody to look closely at this picture and tell me what you see…”
“I see 20 of the world’s top athletes that have tremendous range of motion, strength, body control, and physical capacity… Yet all have significant variances in their static posture as determined by the holy grail plumb-line.
Static posture is near worthless to measure for injury or pain prediction.”
Placing all your eggs into one basket – in this case static posture, which a lot of fitness professionals do – is unfortunate.
Posture is a Position, It’s Not a Death Sentence
To steal from another really smart physical therapist, Dr. Quinn Henoch, “posture will always be relative to two things:
the task at hand
and the load
If you’re not taking into consideration those two things during an assessment – in addition to movement, repetition, speed, etc – and you’re only assessing people based off static posture, well, you’re not smart.
The question, then, is….”what should an assessment look like or consist of?“
It’s not lost on me that the title of this post will raise some eyebrows. The title shouldn’t be taken too literally, because I do feel there are ideal approaches, methodologies, and “rules” to consider when coaching any lift in the weight room.
That said, when it comes to exercise technique (or human movement in general) why are textbooks the metric at which we compare everything?
Textbooks provide context, information, and sometimes make for handy coffee table improvers.
However, we don’t live in textbooks. What a squat, sprint, overhead press (or hell, even a carrot cake) looks like in a textbook can (and usually is) a stark contrast from what is emulated in real life.
I do believe there are some universal tenets to coaching a deadlift or squat or bench press or kettlebell swing8 that will not only allow a client or athlete to marinate in its benefits, but to do so in a fashion that won’t increase their likelihood of injury (or their contributions to their physical therapist’s mortgage payments).
I’m interested in making people savages, but I’m also interested in the long-game. It wouldn’t bode well for business (or my reputation) if all of my client’s deadlifts looked like this:
To that end, with regards to universal tenets for deadlifting:
Loaded spinal flexion is a no-no.
That’s pretty much it.
If you’re following that one golden rule, you’re doing a better job than most. It’s sad, but true.
However, golden rule(s) aside, there are many intricate, more nuanced things to consider person to person. One’s training experience comes to mind. We can’t hold someone holding a barbell in their hands for the first time to the same standard as someone who’s been a competitive powerlifter for 17 years.
Likewise, someone with a vast and delicate history of lower back issues is not going to take the same path as someone with a “clean” health history. And, of course, other factors come into play such as goal(s), movement quality, favorite color, and anatomical/structural differences between individuals.
Someone with hips like this…
…is going to move differently – and presumably be coached differently – than someone with hips like this:
There are many, manyfantastic resources out there that help to break down anatomy, assessment, biomechanics, joint positions, and what’s considered ideal exercise technique. I have my biases as to what I feel is correct – as does everyone – but it’s important to take every resource with a grain of salt, because…
“Textbook technique only exists in a textbook.”
When I heard Mike Reinold say this sentence years ago my immediate reaction was this:
My second reaction was to start doing handstands down the sidewalk outside my apartment, but I didn’t.
You know, cause that’s fucking weird.
And because I can’t do a handstand.
Either way, what Mike said was/is 100% correct.
Textbook technique, in the real world, is every bit as much of a myth as detox diets making you pee rainbows or me riding a Dire wolf to work today
What we read or deem as “ideal” on paper, while often a great starting point for many people, doesn’t always translate to real-life. As coaches it’s important to understand this. Anytime we corner ourselves into one-train of thought or that any one thing applies to everybody, we’re doing the industry – and our clients/athletes – a disservice.
A Real-Life Example
A few months ago I started working with a woman who had been battling some low-back issues, yet wanted to hire me to take over her programming and help clean up her technique.
Specifically she wanted to hone in on her deadlift.
She was frustrated because no matter what she did (or who she worked with), her back always bothered her.
I like to be a fly on the wall and just watch people do their thing during an initial consult. I want to see what their default movement schemes are. In this case I set up a barbell on the floor, loaded it up with a weight I knew she could handle safely, and then asked her to do her thing. Her “default” stance was a conventional stance, and while it wasn’t the worst one I had ever seen, I could clearly see why her back may have been bothering her.
We had established earlier in her assessment that she lacked t-spine extension and her hip mobility wasn’t great either.
More to the point, after doing a simple hip scourand Rockback test, I surmised she was able to attain more hip flexion ROM with more hip abduction. An important point, as you’ll soon see.
Note: the Rockback test is a great assessment to use to figure out one’s “usable” ROM in hip flexion. The idea is to see if or when the lumbar spine loses positioning.
Bad Rockback Test
Notice when spine loses position.
Dead Sexy Rockback Test
Notice the spine stays relatively “neutral” throughout. Also, notice those triceps.
We can then compare what we see here with what we see on the gym floor.9
Going back to my client, she read a lot of articles and books on deadlifting, most of which told her that deadlifting = conventional stance. Always. Moreover, other coaches/colleagues she had consulted with in the past told her to use the conventional stance.
No exceptions.
This is what I mean by falling into the “textbook technique” trap. On paper everything sounds (and looks) great. Everyone can and should be able to conventional deadlift.
In real-life, though…not so much.
Here’s a before and after picture I took of my client. The top picture shows her original set-up with a conventional stance. The bottom demonstrates me putting her into a modified sumo stance.
Immediate improvement in her lower & upper spine position. Having her adopt a wider stance better complimented her anatomy, which then resulted in an infinitely better starting position to pull (no lumbar flexion, improved t-spine extension).
What’s more, with that modification alone she noted there was zero pain.
She left that session feeling motivated and hopeful about training. A win-win if you ask me.
I posted the above picture on some social media accounts – explaining much of what I mentioned above. And wouldn’t you know it: I was called out by a handful of coaches.
One stated the problem wasn’t with her anatomy, but that the real issue was my poor coaching. A funny assertion given he wasn’t in the room with me. Another coach agreed stating something to the effect of:
“No client has walked into “x gym” and not have been able to perform a conventional deadlift after a little coaching on day #1.”
I guess all I could have done at the time was to just go fuck myself.
I demonstrated I was able to clean up someone’s deadlift and do so in a way that was pain-free, and yet, here I was being told by a crew of All-Star coaches I had failed because I didn’t have her conventional deadlift. My actions, apparently, were on par with drop kicking a baby seal in the mouth.
Pump the Brakes
I hope people can appreciate the narrow-mindedness of this type of thinking. To expect everyone to fit into the same scheme or way of doing things because that’s what YOU prefer to do (or because a textbook told you to do so) is about as narrow-minded as it comes.
No one has to conventional deadlift.
Likewise…
No one has to low-bar squat or squat with a symmetrical stance.
No one has to bench press or bench press with an aggressive lumbar arch.
And no one has to start watching Severence on Apple TV. Except, yes you do.
I’d argue a “good” coach understands and respects that everyone is different, and that he or she will be humble enough to put their own personal biases in their back pocket and appreciate there is no ONE way to perform any exercise.
One of the more flagrant “mic drops” I toss down whenever I speak to a group of fitness professionals (remember when we used to be able to do that in person?) is that forcing people to adopt a symmetrical stance while performing basic lifts such as deadlifts or squats is more likely hurting people rather than helping them.
In fact, I’ll go a step further and tell them symmetry in the human body doesn’t exist and then yell something like “UNICORNS ARE REAL!” and walk away.
You’re Not Broken If You’re Asymmetrical. You’re Normal
We need to stop thinking we’re broken if we display any degree of asymmetry.
It’s 100% normal, actually.
The human body is designed asymmetrically. If it were so deleterious I think natural selection would have fixed it by now don’t ya think?
Admittedly, I appreciate it’s a tough nugget to swallow…the whole “symmetry is a myth” thing.
I had a hard time tackling it myself. For years all I read was how we should strive for perfect balance and symmetry both statically (posture) and dynamically (think: maintaining a symmetrical stance during a set of squats).
However, the more I worked with people – with varying backgrounds, injury histories, and body-types – and the more I coached, the more I realized it was all B.S. Holding everyone to the same standard didn’t make sense.
The tipping point for me was my introduction to PRI (Postural Restoration Institute ®) a number of years back. Neil Rampe stopped by Cressey Sports Performance and did a 1-day workshop and opened my eyes to just how UN-symmetrical the body really is.
Not long after Michael Mullin stopped by CSP several times and took the entire staff through a number of in-services which further slapped me in the face with the whole Morpheus “blue pill/rep pill, we’re asymmetrical creatures, open your eyes” schtick.
More currently, guys like Dean Somerset, Dr. Ryan DeBell, Dr. John Rusin, Dr. Stuart McGill, and Papa Smurf agree: The human body is all sorts of effed up.
But in a good way.
In some facets of life symmetry is the goal.
A ballet dancer needs to elicit “symmetry” when performing, as does a figure athlete or competitive bodybuilder when strutting their stuff on stage. No one ever won Ms. Olympia or Mr. East Lansing Stud Muffin with a yoked up right quadricep and a teeny tiny left.
But those examples aren’t necessarily the same thing as what I’m referring to in this post. Aesthetically, symmetry is visually pleasing.
90’s Mariah = pleasing
Crazy Eyes from Mr. Deeds = not pleasing
However, for performance or function, symmetry shouldn’t necessarily be the default goal or expectation.
It’s a hefty statement to make, and whenever I say something so seemingly egregious it often invokes a little push-back.
“Well, what about cars?” someone may blurt out. “If we don’t maintain alignment (symmetry) the car will start veering to one side or the other, causing additional wear and tear on the tires, and run the risk of further damage.”
To this point, I agree. Cars are designed by engineers and manufactured by computers and machines with precise precision to be replicated over and over and over again to (hopefully) ensure a quality product and return business from consumers.
The human body is not a Volvo.
This isn’t to insinuate the human form is any less fantastical, beautiful, intricate, or complex of a design. But, you know, we’re not some Clone Army to be replicated en mass.
Dare I say: This is a rare moment where “we are, indeed, all special snowflakes.”
During our Complete Shoulder & Hip Blueprint (dates are in the works for a return in early 2022!), Dean Somerset and I try to reiterate to attendees that asymmetries are normal and that, often, we’re doing a disservice to our clients and athletes by forcing them all into a standard, one-size-fits-all way of doing things.
It’s important to recognize everyone has variances in bony structure.
Using the hips as an example we know:
Pelvic structures differ person to person.
Femoral angles vary person to person.
Hip socket depth can vary (Scottish hip)
People have two hips (surprise!) and either side can have retroverted or anteverted acetabulums, as well as retroverted or anteverted femoral heads. All of which affects someone’s ability to flex, extend, abduct, adduct, externally and internally rotate the joint.
To that end, when coaching someone up on the squat why not use those variances to better set up your clients and athletes for success?
Much like what an optometrist does when fitting someone for a new pair of glasses, sitting someone down in front of that thingamabobber (<— I believe that’s the technical term) and flipping back and forth between lenses to see which looks and feels better – is this better, or is this? – why is the parallel approach all of a sudden wrong when trying to figure out the best squat stance for someone?
Shouldn’t it be our goal to figure out what stance feels more stable, powerful, and balanced? I’d make the case we’re trying to fit square pegs into round holes much of the time when we force people to use a symmetrical stance.
Why?
Especially when we know there’s a multitude of structural anatomical variance from person to person.
If you’ve somehow developed a mutant power of X-ray vision:
1) That’ll help
2) Can we hang out?
Performing a thorough assessment – something both Dean and I cover in depth HERE (hint, hint) – will provide a ton of feedback and help peel back the onion of what will be the right approach for someone.
You could also watch Dr. McGill take someone through a hip scour here:
I can’t tell you how many times I’ve encouraged someone to use a staggered stance when squatting, or maybe to externally rotate one foot more than the other, and then they perform a few repetitions and they look up and say “holy shit-balls that feels so much better.”
And we hug.
Why would I disregard that?
We’re not causing irreparable harm by accepting asymmetry.
It’s a common tactic for fitness professionals, especially during an initial session or assessment, to go out of their way to demonstrate just how dysfunctional someone is.
“Okay, so, after everything we’ve gone through and discussed it seems you have an internally rotated right shoulder, a bit of anterior pelvic tilt, upper back kyphosis, you lack thoracic rotation on your left side, you need to clip your toenails, and one eye is lower than the other.
We’ve got some work to do to fix everything.”
Now, I’m not going to sit here and say I’ve been perfect my entire career and that I never did the same thing.
I did.
And while hindsight is 20/20…I can’t even begin to imagine how much business I lost because I felt it a good idea to showcase to potential clients how much of a walking ball of fail they were on Day #1.
To that end, I do believe there’s a natural growth or maturation (that only comes with experience) of any fitness professional where you begin to understand and appreciate this train of thought.
Of course it’s our job to “audit” movement and to ascertain, to the best of our ability, what will set people up for the most success possible given their goals, injury history, and ability level(s).
But I adamantly feel that one of the worst things you can do as a fitness professional is to highlight dysfunction and to make people feel broken out of the gate.
Take scapular winging for example, where the shoulder blade lacks congruency with the ribcage (I.e., it peels off the rib cage).
Is it actually a dysfunctional thing?
Now, admittedly, the picture above is a little a lot fucked up.
This is TRUE scapular winging, an actual medical diagnosis where the long thoracic nerve is not doing its job innervating the Serratus Anterior.
No amount of Prone Trap Raises or Forearm Wall Slides is going to fix that dumpster fire. It’s going to entail meticulous manual therapy and someone with a keener sense of neurological wizardry to fix it.
However, many people walk around thinking they have “scapular winging” (HINT: pretty much everyone has it to some degree) and that they’re doomed to a laundry list of corrective exercise purgatory.
I have news for you.
Most people’s long thoracic nerve works just fine and most people are NOT in a state of dysfunction.
In fact you can fix scapular winging pretty quickly by adding LOAD and by getting people to TRAIN.
Load helps nudge people into better positioning and training just helps people not want to jump in front of a bus (trust me: corrective exercise purgatory is no fun for anyone).
There are a litany of ways to accomplish this.
In this short video, I outline some of my thoughts and manage to not swear the entire time.
This is a short clip from mine and Dean Somerset’s new series Even More Complete Shoulder & Hip Blueprint, a brand new product with entirely new content from the version 1 workshop, which is on sale until Sunday for $70 off the regular price, and digs into individualization concepts like this, plus so much more to help you get the best possible plan of action for your clients in order to get them results in the fastest, easiest and safest manner possible.
It’s been a bit, but Part III of Kevin Mullins’ “Corrective Exercise” series is finally here.
I’d sorta mirrors the anticipation everyone had for the Game of Thrones season premiere this past week, except not even close.
Sorry Kev: dragons will always reign supreme over ankle dorsiflexion…;o)
NOTE: Stressing the word “finally” above had nothing to do with Kevin actually writing the article (which he submitted weeks ago), but everything to do with ME and my nincompoopness in actually publishing it.
You are a fitness professional who wants to train people – AKA provide them with enough of a fitness stimulus to generate the results they’ve paid you for. You also want to help them overcome pain and dysfunction in their body.
Thankfully, this series of blogs have got you covered and smothered like Waffle House hash browns.
Which brings us to the final piece of the puzzle – corrective exercises for the knee and ankle.
Many people who would consider personal training deal with some level of knee or ankle problems. In fact, it could be argued that everyone walking around this beautiful Earth has dealt with knee or ankle pain/dysfunction at some point in their lives.
(Tony raises hand. I spent the better part of two years in the early 2000’s working around a cranky left knee.)
A proper discussion of these two joints, one mobile and one stable, would not be complete without a discussion about the role of the hips and feet in the function and performance of the knee and ankle. Our feet are our first and only contact with the ground during much of our lives. Any disruption of their optimal function is going to send dysfunction up the kinetic chain into the ankles and knees.
Just the same, the hip, and its multitude of muscle attachments, functions, and movement possibilities can have a dramatic impact on knee function. Tight hip flexors or imbalanced anterior/posterior chain development can change how the patella tracks over the feet – a recipe for pain or less than desirable movement outcomes. As a proud fitness professional, you should be capable of assessing, correcting, and training clients past many of the common problems that might land on your doorstep.
In this post we’ll explore the anatomy and physiology at play when knees and ankles are the weakness in someone’s kinesiology. We’ll discuss the interplay between the hip-knee-ankle-foot. Then, like the other articles, we’ll discuss five specific issues that most trainers encounter and show off a few new exercises that you can use today.
And then we’ll tie a fancy bow on this corrective series, gather all our jackets and move towards the exits. I hope you’ve found a friend
Basic Knee and Ankle Anatomy – Skeletal
(nerds only)
When looking at the knee joint, we are only considering four specific skeletal structures:
The Femur – the longest bone in the human body is also our primary weight bearing skeletal structure. The femur’s entire function occurs at the hip. It can move through flexion and extension, abduction and adduction, external rotation and internal rotation, and circumduction.
The Tibia and Fibula – load bearing bones of the lower leg. Their design allows for weight transfer in gait and for optimal loading of the lower body during any exercise that creates knee flexion or extension.
The Patella – a bone unlike most others in the body, the patella is interwoven with the tendons that cross the knee joint and serves as a cover for those tendons. The structure of the patella also improves the mechanical efficiency of these tendons.
The ankle joint is a bit more complex though. We must consider the bones of the foot to some degree.
The Tibia – The load bearing bone from earlier is also a major contributor to ankle function. The medial malleolus, a bony growth on the inside of your ankle is located on the tibia. At the ankle, the medial malleolus plays a role in ankle eversion and inversion.
The Fibula – Like the tibia, the fibula is a load bearing bone that also functions during ankle eversion and inversion. It’s bony process, the lateral malleolus, is located on the outside of the ankle.
The Talus – a unique bone in a variety of ways, the talus serves as the base for the tibia and fibula to plant upon. Both dorsiflexion and plantar flexion involve the talus changing position in relation to the rest of the foot. The talus also plays a role in eversion and inversion.
The Calcaneus – connected to the talus via the subtalar joint – the calcaneus functions as a base of support for the structures above it. It hosts insertion points for a variety of muscles and tendons – most notably the Achilles tendon. It is the largest bone of the foot.
(Foot) Metatarsal – critical bone structures that connect the toes (phalanges) to the larger structures of the foot. The metatarsals are critical for weight transfer and distribution and while they don’t move like other bones in the body – their ability to adjust to pressure is critical for elite performance.
(Foot) Phalanges – the toes are the final element of this puzzle. Understanding that the toes can and should flex and extend as a result of ground force reaction or conscious neural action is critical to optimizing the foot’s function. While there may never be a “toe day” – we need to train the function of the phalanges to ensure their relationship with the other foot bones, the ankle joint, and even the knee and hip, are optimal.
Basic Anatomy of the Knee and Ankle – Muscular
It is important to discern the muscles that act on the knee and the ones that act on the hip.
Sure, both are in the thigh and run the length of the femur. However, since the knee joint is designed for flexion and extension – we are only considering the muscles that do just that. With that said, realize that the muscles that do function at the hip must do so properly. Otherwise, the knee joint will act to compensate for dysfunction at the hip and that will cause a host of problems too.
The following addresses strict flexion and extension of the knee joint.
The primary flexors of the knee are:
The muscles of the hamstrings (biceps femoris, semitendinosus, semimembranosus)
The gastrocnemius, popliteus, gracilis, and sartorius are synergistic muscles
The primary extensors of the knee are:
The muscles of the quadriceps (rectus femoris, vastus lateralis, vastus intermedius, vastus medialis)
Now, when looking at the ankle we find simplicity and complexity at the same time. On one hand, there are a bunch of muscles that control the toes and ankle joint that aren’t needed in the typical fitness professional’s vocabulary. Simply put, most trainers don’t need to know the minor details of how the fibularis brevis functions, or where the insertion point of the flexor hallucis longus is.
But they need to know they exist.
(Although, more knowledge is never bad and anyone with an interest in self-myofascial release therapy should understand the interplay between these lesser known tissues).
We do need to know that ankle and foot function relies on many more players than just the prime movers. We do need to understand that dysfunction at the ankle could be a myriad of things and not just a blanket statement about someone’s gastrocnemius.
So, we will address the for major movements of the ankle and point out the muscles for each.
** Take note of just how many more plantar flexors there are compared to dorsi flexors. This could explain why we are so strong with our “calf-raise” exercises and why we typically can access a greater range of plantar flexion under control than we could with dorsi flexion. **
Primary Movers of Eversion
Fibularis and extensor digitorum longus
Primary Movers of Inversion
Tibialis anterior and posterior
When looking at this from a slightly higher viewpoint – we see that we have significantly more muscularity driving both flexions of our ankle joint. The lack of muscularity controlling eversion and inversion explains why we don’t load up on an exercise that challenges that motion. Moreover, it probably explains why “rolling” an ankle can be so devastating – we have so little musculature to control that motion.
Going a little broader, we see that muscles of the lower leg have multiple functions. The tibialis anterior dorsi flexes and inverts the foot while the tibialis posterior contributes to plantar flexion and inversion. The extensor digitorum longus everts the foot while contributing to dorsi flexion. These functions are not accidental – they are essential evolutions and developments of our anatomy to meet the demands of our life.
If we are to succeed in our experience as human beings, then we must be able to communicate with the ground effectively. Thus, the muscles that control our foot, ankle, and knee become our first point of contact with outside world.
Understanding their function, their interplay, and their contribution to elite performance is critical to maximizing the impact you’ll have on your clients and your purpose as a coach.
Basic Movement Physiology
The function of the knee and ankle are highly dependent upon the task we are trying to perform and whether the hips are involved.
For example, the knee will flex and extend during traditional deadlift, but not at the same degree that they would during a front squat. The same logic also applies to the amount of dorsiflexion needed from the ankles to meet that demand.
A different example points to our running stride.
The gait pattern that most elite distance runners take involve very minimal action at the ankles and toes. This sort of “hammer-foot” stride is highly efficient and puts the emphasis on the hips and knees to generate all forward locomotion. Sprinters, however, require maximum action from all the joints of the foot and ankle in order to increase velocity and compete successfully.
Thus, understanding physiology of these structures requires an understanding that optimal function is dependent upon the demands of the task.
Still though, a few notable things exist:
1. When the ankle is in full eversion or inversion – there can be an issue with one’s ability to flex and extend the knee. This is because of the change in position of the inferior aspects of the tibia and fibula creating an up-chain manipulation in their superior aspects (which form the knee joint). It is minor in most but could explain why individuals who live in eversion or inversion find discomfort in their knees.
2. Triple-Flexion (hip, knee, and dorsi-flexion) is the most loaded position of the body because of the major muscles that have created force (tension). In most populations, the greatest power will come from individuals in this position. The stacking of joints lowers the center-of-mass and improves the ability to generate tension.
3. Triple-Extension (hip, knee, and plantar-flexion) is the “tallest” the structures of the lower body will get. The process of going from triple-flexion to triple-extension typically generates the greatest joint velocities.
4. The running stride requires a rhythm between hip-knee-ankle-toe action. Upon foot strike, the toes should flex, which drive the ankle joint into plantar-flexion, assist in driving knee extension, and hip extension. The cycling leg does the exact opposite as it returns to the pre-strike position.
The Major Issues
The knee and ankle joints can be seriously injured during sports and accidents in life. None of the issues discussed below involve torn ligaments, broken bones, or even severe tendonitis. The conditions listed are ones that routinely plague clients who are either inactive or too active with poor function.
In fact, many of the issues of the knee come from overuse of the joint without proper interaction with the hip and ankle. Runners and lifters alike may experience knee pain when their form is off. Likewise, many untrained or detrained individuals deal with knee and ankle dysfunction as a result of their sedentary lifestyles.
And don’t forget about footwear.
There is a cost and benefit to each type of footwear that you and your clients are wearing.
Dress Shoes and Boots – great for making a suit look dapper, or kicking tail on a job site, but atrocious for allowing mobility in the foot. Basically, you feel like you are walking inside of bricks.
High heels – an entire day spent into plantar flexion is not good for anyone. Spending additional time walking in them can hurt the wearer’s ability to distribute their weight once they are out of the heels. Great calves though.
Flip Flops – If you are wearing these, then you are probably at the beach. Sweet. However, that sliding and gliding motion that you are using to keep them on is wreaking havoc on your ankle function while also driving too much knee extension.
O-Lifting Shoes – Having your heels elevated when driving your heavy squats or cleans is awesome – can you say performance? However, if you spend most of your day in these shoes than you can bet your bottom that you’ll begin to lose optimal ankle function since you aren’t feeling the ground.
With all of that said, let’s focus on the five most common things you’ll see in your clients and discuss exactly what is going on.
Lack of Dorsi-Flexion
A lot of people struggle to dorsi flex their ankle in response to loading. In fact, a lot of great coaches, including Tony, have pointed out the importance of adequate dorsi flexion for someone to succeed in a squat pattern.
High quality athletes and desk jockeys can both suffer from this issue. It isn’t simply limited to an inactive or undertrained population. It must be dealt with though if someone is going to optimize the function of their hip-knee-ankle and drive greater results in their programs.
Strengthening the muscles that drive dorsi-flexion while also “stretching” the ankle into these positions with bands or straps is usually the best intervention. We aim to increase mobility, improve strength and stability, and begin providing context and practice with traditional strength training movements such as the squat or lunge.
Runner’s Knee (Patellofemoral Pain Syndrome)
A sort of unofficial name, runner’s knee refers to the over-development of the quadriceps (knee extensors) while also keeping the hamstrings (knee flexors) and glutes underdeveloped. In addition, tightness and exhaustion of the plantar flexors can lead to instability and pain at the knee joint.
In fact, there is some evidence out there that shows that some runners experience a mild shift of their patella in space. Only a few millimeters – this shift can cause significant pain and contribute to the official name of the condition (patellofemoral pain syndrome).
The training for individuals presenting this issue is quite simple:
Release and relax the muscles that plantar flex the ankle and extend the knee.
Strengthen and tighten the muscles that dorsi flex the ankle and flex the knee.
Train the glutes to improve hip drive in the running stride
Traditional strength training and myofascial release typically take care of the problem, although a cessation of running in the short term is almost always a good idea.
Knee Valgus
One of the most misunderstood dysfunctions of “the knee” is a hip issue. Many trainers can coach “knees out” until they’re blue in the face and still get no change in the performance of their client.
First, knee valgus refers to the inability of the hip abductors and external rotators to fire appropriately, thus causing a collapse once tension reaches a certain threshold (such as the bottom of a squat).
Image Credit: prehabguys.com
Now, sometimes this only requires good coaching as the client or athlete simply doesn’t know they are doing it or that isn’t ideal that they are doing it.
We must be wise though. Coaching knees out could be driving excess ankle inversion, which changes the relationship of the tibia/fibula with the knee and could lead to torque being experienced in the knee joint as the body seeks to overcorrect the inversion. This isn’t a common worry – but it is possible.
The training cure though will involve strengthening the abductors and adductors of the hip to improve knee tracking in a variety of exercises. It is important to keep in mind that overtraining the abductors can lead to other problems that only arise when the adductors are forgotten about.
There could also be something going on at the ankle too…
Inappropriate Eversion and Inversion
This one sounds a little silly, doesn’t it?
Inappropriate sounds like someone left their pants at home.
But it points out a deficiency that a lot of people have. Whether it be from a lack of coaching and training, or the development of patterns by accident through sport and training – many people lack the right ankle position to complete the task they are attempting.
Think of that client that can’t stop squatting without eversion. Every repetition pushes them into their toes and insole (often leading to valgus). It could be coaching (or a lack thereof), it could be muscle weakness, or it could be a neural disconnect between their brain and their ankles (they don’t know they are doing it).
Just the same, there are people who can’t seem to run on their big toe. They’ll stride flat footed, especially on the outside of their heels, and wonder why they aren’t getting any better at running. These people have not unlocked enough plantar flexion or awareness of their inversion.
It is exceptionally common to see in long distance runners.
Having the wrong ankle position is coachable and trainable. You must relax what is overused and overworked and strengthen what is left behind. There will be specific protocol for whatever you are seeing. Simply look back at the muscular anatomy and select exercises and interventions that are appropriate.
Disconnect of Hips from Knee/Ankle Function
The final issue that people have with their knees and ankles is that they have no idea they have a pelvis. It is as if they believe their lumbar spine connects to the back of their legs…
No really, you probably have a client or twelve who seem to have no idea how to flex and extend the hips. As a result, everything hurts their knees and ankles. Squatting hurts, running leaves them achy, and they absolutely despise lunges.
They aren’t broken thankfully.
They just need to discover their glutes.
They need to learn how to flex and extend the hip with a lot of exercises that leave the knees out of it. So, deadlifts, hip thrust, banded abductions, Copenhagen side planks, and some anterior core work will do wonders to wake up their hips, stabilize their core, and allow them to excel and knee-dominant and gait patterns. Want to learn more about this? Check out my last installment on the hips.
The Exercises
1. Bulgarian Split Squat to Ankle Glide
https://www.youtube.com/watch?v=2WO3-DQenTI
Your goal with this bodyweight exercise is to create a crossover effect between knee flexion and dorsi flexion. By working with the single leg variation – you’ll enhance your clients focus on one specific ankle while simultaneously exposing them to pause reps for the single leg squat variation. You can train them and correct them at the same time.
2. Banded Dorsi to Heel Raise
https://www.youtube.com/watch?v=qrMjjZKkQ8Y
Great for runners and athletes, but effective for everyone, this ankle exercise only requires a band and a seat.
The goal here is to maximize both dorsi flexion and plantar flexion in the same movement cycle. This sort of training allows for you keep the muscles that control both actions in relative balance. This is not unlike being on a calf raise machine and allowing your heels to dip below the step.
3. Barbell Hip Thrust w/ Banded Abduction
One day I want to call Bret Contreras and thank him for his research on the glutes. (Although this video is of Ben Bruno – a stud coach in LA who does NOT like burpees). Discovering that the hip thrust provides more activity of the glute muscles than other exercises is critical for the development of aesthetic and athletic glutes.
Adding in the abduction component at the top is a sure-fire way to ensure your “knees-out” coaching cue for valgus hits home. The band ensures they move from the hip joint instead of just torqueing at the knees. Add in the isometric hold of the glutes and you’ll be sure to work the hip component of knee stability.
4. Duck Walks
https://www.youtube.com/watch?v=beIn56rJGmU
This is an absolute torture device. Duck Walks, loaded or unloaded, drive the body into that triple-flexion position we discussed earlier in the blog. This coiled position strengthens the posterior chain and improves dorsi-flexion by keeping our feet in a set position.
A highly integrated exercise – the duck walk can be used for neural prep or as a burn out after your primary work is done. Sure, its goofy and it doesn’t “seem” like it is going to do your body any favors, but try it and feel how your systems work together to hold isometric tension.
5. Reverse Nordic Curl to Nordic Curl Superset
https://www.youtube.com/watch?v=H-WpX-dnBuY
We want the quadriceps and hamstrings to be in relative balance for optimal knee function. Depending on our choice of sports or training – one may overpower the other a little. That discrepancy though shouldn’t be a chasm.
Hitting both versions of the Nordic curl in a single superset provides an opportunity to train the muscles in a unique way using only bodyweight.
BONUS: Sprinting
https://www.youtube.com/watch?v=3YqQum4emVw
The act of sprinting is one of the most athletic things the human body can do. The whole body must get in on the act if we are to excel.
Specifically, for the knee and ankle, sprinting helps drive a low-level of eversion while demanding quality cycles through plantar flexion and (mild) dorsi flexion and knee flexion and extension. Add in the function at the hip and we’ve found the perfect lower body exercise for improving someone’s function and interplay between these regions.
Obviously, not every client could sprint or should sprint. Be wise with your prescriptions and coach who you are with, not who you wish they were.
Finding the Exit
So, once again we conclude that we can intervene in our client’s discomfort and dysfunction with exercises that not only correct issues, balance muscles, and improve coordination, but also drive a fitness stimulus.
The knee and ankle are interesting joints in a sense that they have less muscle mass around them than the hips and shoulders. But that doesn’t make them any less important. In fact, their proximity to the ground – a constant in our lives – makes them more important than most trainers think. Everything that is dysfunctional at the foot, ankle, and knee will run up the chain into the hips and spine and even the shoulders.
Help your clients discover their foot stability, ankle mobility, and knee stability and you’ll help them discover a better body – both in performance and in aesthetics.
Thank You
Thank you for your time.
Thank you to Tony for allowing me to share my ideas on his website – a treasured space on the internet.
Whether you visit him for his pop culture references, his biceps veins, or his absurd level of knowledge about the body – you’ve made a great choice.
I truly hope you have learned something from this series and enjoy my writing style. I poured a lot into this, and into my book, Day by Day. I hope I can download everything I have learned (good and bad) from me to you every chance I get.
Like I say to my clients, “let’s get just a little bit better every day.”
Check Out Kevin’s Shit
You can read more of Kevin’s stuff at his website HERE.
Just to help calm the waters: I am not anti “corrective exercise.”
And I am not really going to throw my face into a brick wall.
I respect and can appreciate that, sometimes, our jobs as fitness professionals require us to pump the brakes and to venture down the corrective exercise rabbit hole.
Some people require a bit more TLC with regards to improved movement, motor control, and/or, and I’m paraphrasing here…”just learning to turn shit on.”
Some people will require a laundry list of additional mobility work, stretching, or positional breathing drills to point them in the right direction and to help them feel better.
What I am against, though, and what drives me bonkers, is when coaches and personal trainers go out of their way to:
1) Overstep their scope of practice and end up performing really shitty physical therapy with their clients and athletes.10
OR
2) Highlight every minor “dysfunction” with a client/athlete – excessive anterior pelvic tilt, kyphotic posture, left eye is lower than the right (you freak) – making him or her feel as if they’re walking ball of fail.
Here’s another gleaming example of how TRAINING is corrective and how, if we do our jobs as coaches, we can often accomplish a lot sans the brick wall.
My client, Emily, who’s a trainer herself, has been dealing with some left shoulder issues. I had her come in the other night to see if I could offer some insights and to listen to some sick EDM beats.
The latter has nothing to do with anything, but whatever….give THIS a listen.
Emily showed up and I took the picture below. It shows something clearly awry and that some sort of shoulder clusterfuckey was at play; namely lack of shoulder flexion on the left side.
What was the culprit?
It could have been a few things:
Capsular issue
Lack of scapular rotation (namely upward rotation).
Soft tissue restriction.
Lack of lumbo-pelvic control.
It was a Wednesday.
I don’t know.
What I do know is that I had to respect my lane and understand it wasn’t my job as a strength & conditioning coach to diagnose anything.
I could, however, assess her general movement capacity, use my knowledge of anatomy, and perform a little trial and error to see if I could improve things.
What follows is more or less a brain dump and an attempt to explain my thought process as I worked with Emily for the next hour.
I’m not gonna say that what ended up happening was on par with some Matrix level shit, but I will say I basically know Kung-Fu.
“What actions have to happen at the scapulae in order to get the arms overhead?”
– Upward rotation
– Protraction
– Posterior tilt
Emily wasn’t getting much upward rotation on that left side. When I asked her to bring her arms overhead it was as if her left arm hit a massive speed bump and came to an abrupt stop. She could push through it, but not without pain.
So I had to think about what muscles help with that action (upward rotation)?
– Upper and lower traps
– Serratus
Too, I noticed she also had a more depressed shoulder girdle as a whole; her clavicular angle was more horizontal rather than having a slight upward grade.
HERE‘s Eric Cressey discussing this in a little more detail.
I surmised her UPPER traps needed some attention.
The upper traps often get a bad rap and are avoided like a Coldplay concert. In certain populations (think: desk workers) and instances, the upper traps are OVERactive and can play a role in increased shoulder elevation as well as superior migration of the humeral head, and hence an increased risk for shoulder impingement.
In this scenario, it behooves us to not go out of our way to increase upper trap activation.
However, we often forget the upper traps are a major player in UPWARD ROTATION, not to mention help with scapular elevation…both of which, in my eyes, Emily could have used some more of.I didn’t get over corrective with Emily and start having her perform some voodoo like tapping her pinky finger three times while flossing her teeth with a strain of hair from a Hippogriff.
I didn’t have her perform a laundry list of “correctives” that, for all intents and purposes, would have likely made her feel like a patient and bore her to tears.
Nope, I had her TRAIN and just modified a few things.
We did:
1. Landmine Presses with a Shrug/Reach
2. Face Pulls in an upwardly rotated position (so the upper traps were more engaged)
3. And, instead of performing movements that would pull her into more shoulder depression and downward rotation (deadlifts, farmer carries, etc) we opted for Landmine Squats, Zercher RDLs, and Hip Thrusts.
In short: We turned shit on (upper traps) and trained movements that (likely) wouldn’t feed into the root causes of her symptoms.
Here’s the picture I took at the end of her session:
When it comes to neck pain, as a strength coach, I (generally) don’t touch that with a ten-foot pole. It’s case dependent of course, but more often than not, if someone I’m working with walks in with a some significant discomfort in their neck I 1) start hyperventilating into a paper bag and 2) immediately refer out to a someone who has more diagnostic and manual therapy skills.
This is not to say, however, that there aren’t any avenues to take if you’re a personal trainer or strength coach. It’s not like you can’t do anything. In today’s guest post physical therapist, Dr. Michael Infantino, goes into great detail on some things to consider if you ever find yourself in this predicament.
The Gym Is a Pain In My Neck: Two Movements To Cure Them All
Are you struggling with neck pain?
Does the gym make it worse?
Do you find yourself looking at a lot of informative websites for ways to resolve these issues, but wish it were compactly put in one place?
Does this sound like an infomercial?
Well it’s not!
But for just $29/month you can… just kidding.
This article is here to solve all of those problems. Neck pain is often blamed on poor form when exercising. This is absolutely true. Unfortunately this does not answer a crucial question, “why?” Discovering WHY your form is poor is the goal. On top of that, people often fail to recognize other human errors that are contributing to their symptoms. We will provide a guide for figuring out why you have neck pain and how to resolve it.
In most cases, pain attributed to the gym can be tied to the following:
Limitations in the necessary mobility to perform a movement
Limitations in the skill needed to perform a movement
Limitations in the capacity to perform a movement (Strength and Endurance)
Human error [Electrolyte and Fluid balance, Self-Care, Rest, Sleep, Breathing, Posture, Medication and Fear.]
Limitations in MOBILITY: 2 movements to cure them all!?
Limitations in your ability to put yourself in optimal positions during almost any upper body movement are a result of two movement limitations.
Limitations in these positions can lead to a host of different complaints. For the sake of time we are going to pick on NECK PAIN. If you are struggling with one exercise you are likely struggling with another, you just might not realize it.
Position #1: Shoulder Extension Test
Movements: Push Up, Pull Up, Row, Dip, Pull Up (top), Jump Rope, Punching someone in the nose because they have one of those weird miniature poodle mixes.
Attempt to perform the ^^THIS^^ motion
Instructions: Keep the neck retracted while extending the shoulders just beyond the trunk without the following:
Increased forward head position
Forward shoulder translation
Shoulder shrug
If you are unable to replicate the picture above you likely have a MOBILITY problem.
If you can’t perform this motion when you aren’t under load, you will definitely struggle when you are. Especially with repeated repetitions and the addition of weight.
Target Areas for Treatment
Soft Tissue Mobility
Pecs
Serratus Anterior
Upper Traps
Stretches and Joint Mobilization
Chin Retraction
Thoracic Extension (arms overhead)
Open Book Stretch
After working these bad boys out I want you to RE-CHECK the test position.
Is it better?
If not, you need to keep working on it.
Assuming you now have the necessary MOBILITY to perform this motion, we need to make sure you have the required SKILL with the particular movement you are interested in.
Skill: the necessary strength, stability and coordination to perform the most basic form of a loaded movement (pull up, push up, dip, row, etc.).
Are you able to maintain a good position in the:
Bottom of your push up
Row
Top of your pull up
Bottom of your dip
Jump roping
As you load the arm for a hay maker!
We aren’t as complex as you might think. Many of our daily activities are broken into a few movement patterns.
Follow this sequence:
Create the mobility necessary to perform the pattern in its most basic form. (In this case, Position #1 and #2).
Ensure you have the skill needed to perform your desired movement (Push Up, Pull Up, etc.)
Build capacity with that movement (Endurance and Strength).
If you don’t have the skill to perform a specific exercise or movement, you need to practice. Look at the above definition of skill to make that judgement. If you don’t have the baseline strength to perform one good push up, pull up, dip or row, see below for regressions that will allow you to maintain good form as you work your way back to mastering these moves.
Here are some ideas:
Push Up: Inclined position (Ex. against weight bench or counter), knee push ups
Pull Up: Assisted with a band, inverted row
Dip: Assisted with a band, bench dip
Row: Kind of an outlier since this move typically doesn’t require body weight. Use a weight that allows good form. TRX Row and inverted row are body weight options. Adjust the angle of your body to reduce the difficulty.
The goal here is to demonstrate the ability to maintain proper form throughout each movement with a regression that is appropriate for you.
Joe Muscles next to you may need to take 50 lbs. off his 200 lb. weighted belt during his pull-ups to maintain good form. You may need to work on getting one pull up with good form without any extra weight.
Most of us have one or two good pull ups in our bag of tricks to whip out for an “impromptu” Instagram post. Preventing injury is going to require you to build the strength and endurance to exceed Instagram’s one-minute time cap. DAMN you Instagram!
Adding repetitions and weight to the regression will help you work your way back to a standard pull up, row, dip, push up, etc.
I can’t emphasize this point enough.
We all have high expectations of ourselves. Neck pain after 10 reps is not necessarily a “push up” problem. It may be the fact that you did three other exercises before push ups that started to fatigue the neck. The push up was the breaking point. You need to have a realistic expectation of your current ability, or capacity.
Position #2: Overhead Test
Movements: Overhead Press, Pull Up (bottom position), Snatch
Instructions: Lie on your back with knees bent. Tuck chin (neck flat to ground) with arms flat to the ground in the start of a press position. Press arms overhead by sliding arms along the ground.
Common Faults:
One or both arms come off the floor at any point in time.
Compensatory forward head or extended neck position to keep arms on floor
Compensatory spine arch to keep arms on the floor
Assuming you repeatedly tried to replicate this position without success, once again we have a MOBILITY PROBLEM.
Target Areas for Treatment
Soft Tissue Mobility
Pecs
Lats
Rhomboids
Stretches and Joint Mobilization
Chin Retraction
T-Spine Drop In (or T Spine Extension)
Open Book Stretch (Add: External Rotation at Shoulder)
1st Rib and Scalene mobility
After finding the weak link, it is time to RE-CHECK. If it looks better, great let’s move on. Similar to Position #1, assuming you now have the pre-requisite MOBILITY to perform this motion we need to make sure you have the SKILL necessary.
*If you are having trouble improving your mobility or resolving pain, seek the advice of a qualified medical provider or fitness professional.
Can you maintain the same control and form during your overhead press, snatch, hang position of your pull up (or any variation- kipping pull up, toes to bar)? If not, we need to REGRESS the move. Unlike the shoulder extension position, many of the overhead exercises can be regressed by reducing the weight or working on single arm presses instead of two arms. Other regressions include:
Regressions:
Overhead press: Landmines (Tony goes into more depth in this article).
Snatch: Cleans, Single arm overhead kettlebell squat, single arm overhead lunge
Pull up (bottom): use a resistance band for support, inverted row
Human Error
Now that you have mastered Position #1 and #2, it is time to make sure that you are limiting HUMAN ERROR.
I think everyone should have someone in their life that serves as an extra pair of eyes. Even the best fitness trainers and medical providers in the world have a hard time being objective toward different areas of their own life. Barbers don’t cut their own hair, right? Not positive about that one. Either way, you can’t go wrong with some quality feedback!
Most of us are quick to blame the boulders in our life when it comes to pain, but we overlook the pebbles.
With pain we can’t overlook the pebbles.
The pebbles are diet, water intake, sleep, and self-care habits.
Patients usually tell me that they are doing “better than most” or that they are “pretty good” about optimizing these areas of their life. It isn’t until their spouse shows up to the appointment that we get the whole truth.
I love it!
Proper Fluid and Electrolyte Balance
Paying attention to what you consume pre and post workout is important. Proper fluids and electrolyte intake prior to exercise can help delay muscle fatigue and cramping.
Many people can get by with less than optimal effort when it comes to this category. However, if you are having neck pain you need to give yourself the best chance at success.
“At least 4 hours before exercise, individuals should drink approximately 5-7 mL·kg−1 body weight (~2-3 mL·lb−1) of water or a sport beverage. This would allow enough time to optimize hydration status and for excretion of any excess fluid as urine” (Sawka, 2007).
This is not always possible, I understand. Do your best. Some is better than none.
Warm Up
Proper warm up is also important.
Engaging in a warm up that gradually increases heart rate and muscle flexibility is a great way to prime the muscles. Dramatic increases in blood pressure and heart rate can lead to less than optimal muscle performance and increased risk of exertion headache during your workout.
Your warm up should be focused on getting the heart rate up; along with preparing the body for the movements you are going to perform during your workout (squat, push up, deadlift, clean, etc.).
Taking the time to stretch and do some soft tissue work after exercise will help reduce muscle soreness in the days following your workout (Gregory, 2015).
Leaving your body more prepared for the next workout. It is a great way to improve muscle extensibility and eliminate trigger points that aren’t allowing your muscles to perform effectively (Lucas, 2004).
Adequate rest is also important for recovery.
Going hard every day and not getting adequate sleep does not allow your body to grow and repair itself. Neglecting proper recovery leads to a less than optimal immune system and central nervous system.
Sleep deficits can also lead to an increase in the intensity of pain and alterations in mood. This is some serious shiznit. Can’t express enough how important this category is. I am a huge fan of the “grind.” It just sounds cool. You aren’t meant to grind everyday though, so please take some time to recover.
Breathing and Posture
Proper breathing is something that is often overlooked, but may be contributing to neck pain.
Gritting it out is cool, I highly recommend it. It builds character.
However, regularly holding your breath or clinching of your teeth when exercising can lead to increased tension around the neck. This could end up resulting in tension headaches as well.
Many of us without realizing it spend most of our day performing shallow breaths. We often over utilize the neck musculature. Shallow breathing into the chest can increase tension in these muscles and even increase feelings of anxiety.
It is recommended that people learn how to perform relaxed diaphragmatic breathing to reduce tension in the neck muscles. Staying in sustained postures throughout the day can also be contributing to your neck pain.
Many studies continue to show that sustained postures throughout the day (typically with office workers), especially with a forward head position, can increase neck pain and headaches (Ariëns, 2001).
Symptoms are also more common in people that hate their job.
Really off topic, but it is true …
Consider how stress in your life (emotional or physical) is amplifying your feelings of pain. Emotional pain and physical pain are HEAVILY connected. Check out this video by Tony to learn a little more about proper breathing strategies.
The Advil Fix
This may not seem to fit with the other categories.
Nonetheless, it is super important.
Side effects related to over the counter anti-inflammatory use are becoming common knowledge. Every now and then I run into someone that isn’t aware of the potential risks of regular use.
Popping over the counter anti-inflammatories (i.e. advil) before or after your workouts IS NOT recommended.
It’s like sweeping the dirt under the rug.
“The most common side effect from all NSAIDs is damage to the gastrointestinal tract, which includes your esophagus, stomach, and small intestine. More than half of all bleeding ulcers are caused by NSAIDs, says gastroenterologist Byron Cryer, MD, a spokesperson for the American Gastroenterological Association.”
Fear
One of the reasons that I started RehabRenegade.com was to help share information like this with as many people as possible. Many of the complaints I get in clinic can be fixed SUPER QUICK. Having a basic understanding of how to care for yourself and knowledge of the body can remove the “threat” of pain.
Red flags (serious pathology) represent less than 2% of the cases that are seen in a clinical setting (Medbridge, Chad Cook: Cervical Examination).
The Internet can be a blessing and a curse.
It can either lead you down the right road or scare the living crap out of you. We all know that any injury or illness is usually presumed to be cancer after a late night search on WebMD. Here are some discussions and advice I found on the inter-web related to neck pain in the gym.
Great intentions, but poor advice.
We tend to blame everything on a “pulled muscle,” whatever that means.
Rest?
What year is it?
We stopped recommending straight rest in like 1902.
By all means, take time off from the gym.
This doesn’t give you free rain to lie in bed all day watching re-runs of Game of Thrones.
It’s true… you may have over done it. Your muscles were overworked. Likely leading to a nice amount of local inflammation and some trigger points. The more constructive advice would be to perform some soft tissue work, light stretching and low intensity non-painful exercise to keep that area mobile.
Resorting to pain medication is not a healthy option. Last but not least, mentioning damaged discs and compressed nerves never makes someone feel at ease. Trauma to the neck may be a reason for disc injury. Overdoing your push ups and pull ups is NOT.
Fun Fact: The prevalence of disk degeneration in asymptomatic (without symptoms) individuals increased from “37% of 20-year-old individuals to 96% of 80-year-old individuals. Disk bulge prevalence increased from 30% of those 20 years of age to 84% of those 80 years of age” (Brinjikji, 2015).
Positive findings on MRI are common in people without pain. Don’t get too caught up in images and diagnoses. Do the things we know are healthy. If you hit the gym hard this morning and then followed that up with a CROISSAN’WICH from Burger King, and a cigarette at lunch we have bigger fish to fry.
First and foremost, muscle and joint strain at the neck commonly refers pain to the head. We call this a cervicogenic headache. Rest assured that it is very rare that you have a more serious pathology requiring immediate medical attention. Give the tips in this post a shot, if it doesn’t help by all means see a medical professional. The worst thing you can do is show up to your medical provider without attempting to improve your flexibility, tweak your form or get adequate rest.
If I had a dollar for every time a therapist told someone they had the tightest (fill in the blank) they have ever seen I would be a little better off.
If this poor girl wasn’t worried enough… Now she has the tightest back he has ever seen… really?
As providers we need to be very careful with our words. It is really easy for us to turn neck pain into chronic neck pain.
It is called an iatrogenic vortex.
When people get tied up in the medical system too long they often see symptoms worsen or develop other unexplained diagnoses.
Overview
In most cases, pain attributed to the gym can be tied to the following:
Limitations in the necessary mobility to perform a movement
Limitations in the Skill needed to perform a movement
Limitations in the Capacity to perform a movement (Strength and Endurance)
Human Error [Electrolyte and fluid balance, Self-Care, Rest, Sleep, Breathing, Posture, Medication and Fear]
You could be one small modification away from eliminating your neck pain.
The big takeaway here is to make sure you have the ability to perform various exercises with good skill.
From there, you need the knowledge and self-awareness to know when you have exceeded you capacity.
You also need to look at the big picture to ensure that you are checking the boxes when it comes to living a healthy life. If you are someone that often finds yourself worried or anxious when injury sets in please take a step back and look at the big picture. Use this article to see where your gaps are. If you still can’t get relief please see a medical provider. Nothing makes medical providers happier than working with patients who demonstrate a willingness to learn and grow.
About the Author
Dr. Michael Infantino is a physical therapist. He works with active military members in the DMV region. You can find more articles by Michael at RehabRenegade.com.
References
Ariëns GAM, Bongers PM, Douwes M, et al
Are neck flexion, neck rotation, and sitting at work risk factors for neck pain? Results of a prospective cohort study. Occupational and Environmental Medicine 2001;58:200-207.
Brinjikji, W., Luetmer, P. H., Comstock, B., Bresnahan, B. W., Chen, L. E., Deyo, R. A.,Jarvik, J. G. (2015). Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. AJNR. American Journal of Neuroradiology, 36(4), 811–816. http://doi.org/10.3174/ajnr.A4173
Gregory E. P. Pearcey, David J. Bradbury-Squires, Jon-Erik Kawamoto, Eric J. Drinkwater, David G. Behm, and Duane C. Button (2015) Foam Rolling for Delayed-Onset Muscle Soreness and Recovery of Dynamic Performance Measures. Journal of Athletic Training: January 2015, Vol. 50, No. 1, pp. 5-13.
Lucas KR, Polus BI, Rich PS. Latent myofascial trigger points: their effects on muscle activation and movement efficiency. J Bodyw Mov Ther. 2004;8:160-166
Sawka MN, Burke LM, Eichner ER, Maughan RJ, Montain SJ, Stachenfeld NS. American College of Sports Medicine position stand. Exercise and fluid replacement. Med Sci Sports Exerc. 2007;39:377-90.



























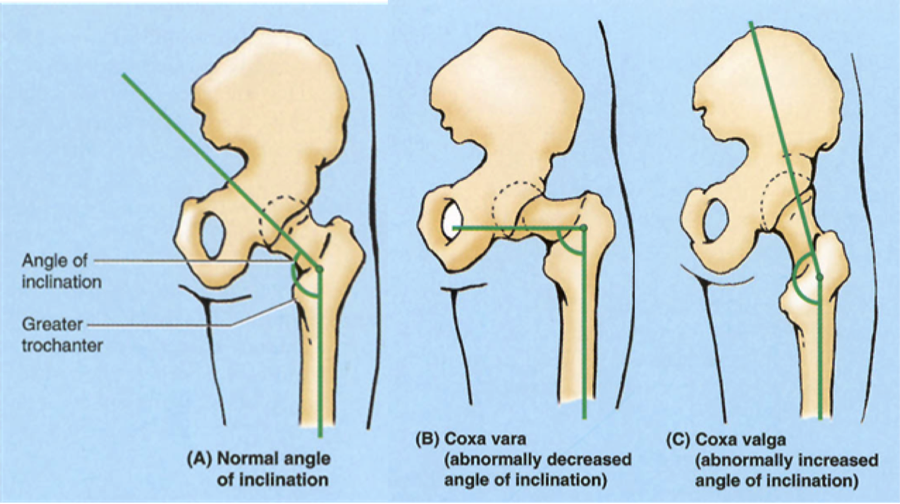













 Dr. Michael Infantino is a physical therapist. He works with active military members in the DMV region. You can find more articles by Michael at
Dr. Michael Infantino is a physical therapist. He works with active military members in the DMV region. You can find more articles by Michael at 

