Today’s guest post comes courtesy of TG.com regular, Travis Hansen.
It mirrors a sentiment I’ve been championing for a few years now: That we don’t have to start hyperventilating into a paper bag the second we notice asymmetry in our clients/athletes.
It behooves us to maybe lean into it a bit more.
Not always, of course. But certainly more often than we think.
I’m sure there are many who read this article title and immediately wanted to grab their pitchfork.
Hear me out.
There are many times when you actually need to embrace the notion that our body’s natural anatomical design consists of several structural asymmetries perfectly balanced to allow us to perform at a higher level.
Cue dramatic chipmunk here.
https://www.youtube.com/watch?v=a1Y73sPHKxw
Moreover, there are even times when you can implement an imbalanced approach both through a direct exercise, but also through how much volume you incorporate, to help neutralize a dysfunction that currently exists.
And lastly, even in the presence of elastic/power, strength, and even limb length disadvantages, the body routinely seeks a way to remain healthy and perform at a higher level.
Note From TG:If you’re interested, HERE‘s my take on why leaning into asymmetry is likely the right branch to bark up.
Lets take a look at the first element of asymmetry that exists in the human body beginning at the foot.
I don’t think anyone would argue at this point that the various plantar flexors of the foot responsible primarily for propulsion in human movement vastly out-weight and out-perform the smaller and less powerful dorsiflexors of the foot.
Why would this be the case though?
If one group, which primarily lies on the backside of the lower leg, dominates the front side of the foot, wouldn’t there be tearing that would occur on the front eventually regardless of how much of an attempt to balance the leg is achieved?
The shin muscles do indeed tear from (mainly) eccentric overload and weakness but this can be solved.
Regardless, a balance exists at the lower leg just like many other areas, and there is just enough size and strength present in the leg in healthy individuals to allow this imbalance to occur without any problems.
Another example, can be seen at the shoulder.
Consider that your Latissimus Dorsi, teres major, biceps, anterior deltoid, and pecs all have the capacity to drive the shoulder into horizontal adduction and accelerate the arm explosively, while everything on the backside, which isn’t much, is stuck with the job of having to slow this arm action done.
Of course, the posterior muscles will fail to match the strength output of the powerful anterior shoulder group.
However, we’re designed pretty miraculously.
Our shoulder, specifically the posterior cuff, can slow “things” down just enough to bridge the large gap between front and backside and allow us to remain healthy and continue to increase throwing velocity without much issue.
Note From TG: Another way to think of it is that if the body WAS designed symmetrically or if we went out of our way to seek it, that would likely inhibit an athlete’s ability to throw a baseball in the first place. As a thrower throws, particularly at a young age, there’s a bony adaptation that occurs (retroversion) which then allows for an aggressive layback position to throw a baseball faster and faster.
If we tried to “fix” that or if the body was designed to be “equal” we’d have a lot of 72 MPH fastballs out there.
Of course, this isn’t to say there aren’t certain training modalities and manual therapy approaches we can implement to help “offset” this imbalance; there are many.
That being said, from an athletic development standpoint, the late Charles Poliquin even pointed out that elite sprinters carried a much more powerful posterior chain than anterior chain in attempts to sprint faster.
Charles declared a 100% ratio, but whether or not that figure is valid remains unseen.
To support his statement and raw figures aside, the body cannot run faster after initial phases of sprinting since vertical forces stagnate and any further increase in running speed stems from increased hamstring, glute, and horizontal force production.
The Second Layer of Asymmetry
The next example where we can begin to appreciate imbalances deals with a particular approach to program design in those people with “severe” asymmetries.
Take an anterior pelvic tilt for example.
If this message hasn’t been driven into your brain enough already, it’s worth repeating one more time since its still so prevalent:
…and that is utilizing a pre-dominant training ratio hip to quad exercises.
There is naturally a slight lordosis and anterior pelvic tilt that does and should exist in athletic and power-based postures, but excessive imbalance is what becomes problematic. The same scenario can be seen at the shoulder like was previously mentioned, anterior versus posterior core, and in other planes of motion as well.
Along these same lines, you will see training tactics such as RNT, PAILs, and RAILs all seeking to address imbalances by subtly or substantially inducing imbalances.
Alwyn Cosgrove first coined the idea of creating an imbalance to cure an existing one.
For example, if you present with a common lateral weight shift during a squat you can actually add increased poundage towards the side of the shift or set up a resistance band to pull you in that same direction to built an instinctive reflex to get you back towards center.
More importantly, it will create a tactile awareness of the issue that you will have memory of in the future in case that same issue decides to manifest again and you will know precisely how to correct it.
Third Layer of Asymmetry
Lastly, is the issue of seeking to reduce or even eliminate according to some, the effect of having one limb stronger or more powerful than the other.
In the most extreme cases, you can witness the damaging effects of strength discrepancies with common orthopedic evaluations such as the 90 degree isometric lateral raise test.
It’s been stated that if there is a strength imbalance or pain response that results in one arm being over +50 percent stronger than the weaker arm that could be indicative of a full thickness tear to the supraspinatus muscle.
So yes, there does need to be at least some balance or an attempt to balance out joints for an athletic performance standpoint to prevent scenario’s such as this one.
But is it fair to ever think that we could actually fully restore joint strength so that we are equally strong everywhere?
No.
1) For the reasons that were mentioned earlier based on our anatomical design, and 2) you just won’t see it happen.
If you truly test single leg strength with optimal testing selections such as pistol/single leg squats, or Bulgarian drills for strength capacity, or advanced bounding plyometric variations for power, you will witness differences in volume, endurance, and intensity more times than not.
A handful of my coaching colleagues have been posting rad videos recently of their young athletes doing rad things.
On a final note, consider that Usain Bolt has one leg that is inches longer than the other but contributes to key characteristics of sprinting speed, and this notion of imbalance is further perpetuated.
Maybe it’s time we start to look at imbalance differently when necessary and start embracing the notion rather than trying to erroneously fight it, and see what happens.
About the Author
Travis Hansen has been involved in the field of Human Performance Enhancement for nearly a decade. He graduated with a Bachelor’s degree in Fitness and Wellness, and holds 3 different training certifications from the ISSA, NASM, and NCSF.
He was the Head Strength and Conditioning Coach for the Reno Bighorns of the NBADL for their 2010 season, and he is currently the Director of The Reno Speed School inside the South Reno Athletic Club.
He has worked with hundreds of athletes from almost all sports, ranging from the youth to professional ranks. He is the author of the hot selling “Speed Encyclopedia,” and he is also the leading authority on speed development for the International Sports Sciences Association.
Kevin knows how to train hockey players. However, the information below can be applied to any athlete. In short: when it comes to making someone faster the answer is rarely “just go do some sprints.” Digging deeper and understanding inherent limitations from athlete to athlete needs to be considered.
Speed is one of the most highly coveted physical attributes in almost any sport, but particularly in ice hockey.
Unfortunately, many speed development programs take a bunch of dynamic warm-up and sprint exercises from track and field, scramble them together, and assume players will get faster.
There are two fundamental flaws in this line of thinking.
First, there is a lot more to speed development than simply sprinting.
Second, the assumption that all players (regardless of age, training background, physical development, etc.) will respond favorably to this type of program is clearly misguided.
The “this is what most people need” logic leading to this type of program is unique to the fitness industry and clearly unacceptable in almost every other area. For example, can you imagine picking your car up from a mechanic, and having he/she tell you…
“I rotated your tires, changed your oil, and topped off your windshield wiper fluid.”
“Why’d you do that?”
“Well that’s what most people need.”
“Yes…but I came in because my car is leaking transmission fluid.”
Having a diagnostic system to help identify limiting factors to speed development will help you avoid both of these mistakes by providing clarity on which physical qualities need to be the focus of a training program, and by tracking progress to ensure the training is actually leading to the results you desire.
Limiting Factors to Speed Development
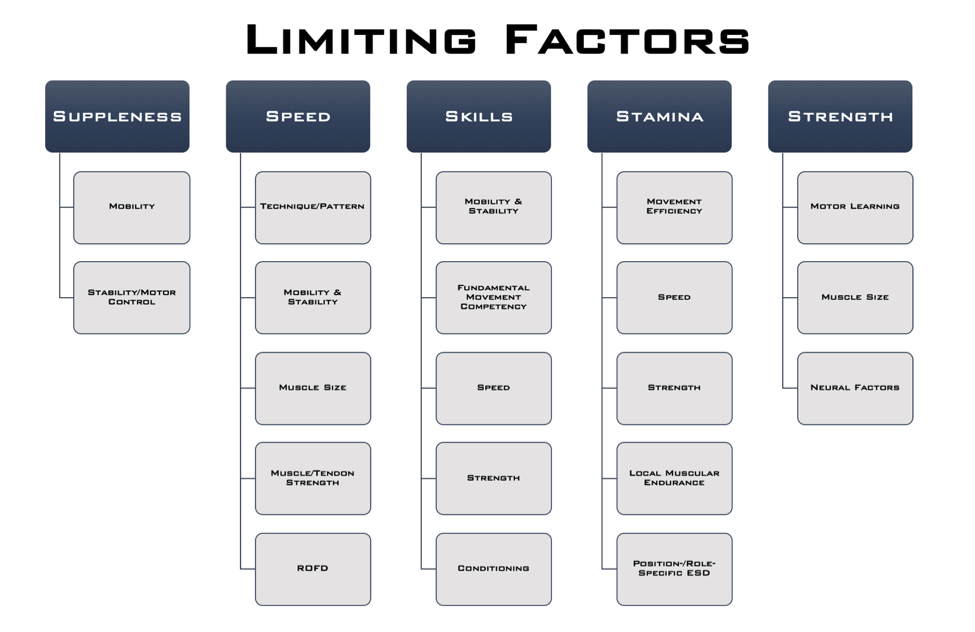
Below is a slide from a talk I gave at the NSCA’s Training for Hockey Clinic a few years ago. While this is overly simplistic, it provides a starting point for understanding the key elements that underlie performance in each area, and therefore what areas need to be “tested.”
Focusing in on speed, there are 4 key areas that contribute to speed development and expression.
1. Technique/Pattern
Speed can be limited by a player’s technique or skating pattern. This is why skating coaches are so important – if players aren’t taught to skate efficiently, to find their optimal skating depth, feel comfortable on their edges, learn optimal transition mechanics, etc., they’ll inevitably be wasting energy and skating slower than they could if they improved their mechanics.
2. Mobility/Stability
That said, from an off-ice training perspective, one of the major goals of training is to remove barriers that may be preventing a player from skating with optimal technique, which brings us down to the rest of the items on this list.
From a mobility standpoint, if a player doesn’t have the ankle and hip mobility to get into an optimal skating position and execute an effective stride, they’ll be leaving speed on the table.
In support of this concept, Upjohn et al. (2008) compared the skating patterns of high and low caliber players, and found that high caliber players set up with their hips, knees, and ankles all flexed more, and this allowed them to have a longer and wider stride length, and greater knee and ankle extension during the push-off phase of skating. In other words, a lower skating position translated into a longer stride length, which allowed for a more powerful push-off with each stride.
In this way, ensuring that the player has the adequate range of motion to get into a deeper skating position can be viewed as speed training.
This research is insightful because it highlights the importance of having adequate ankle mobility. A lack of dorsiflexion, or knees going over the toes, will limit your skating depth, and a lack of plantar flexion, or pointing the toes away from the ankle, will limit your power through the end of the push-off. What isn’t as readily apparent, is how a deeper skating stance will require increases in other components of hip mobility, notably hip abduction or moving the foot out to the side away from the hip.
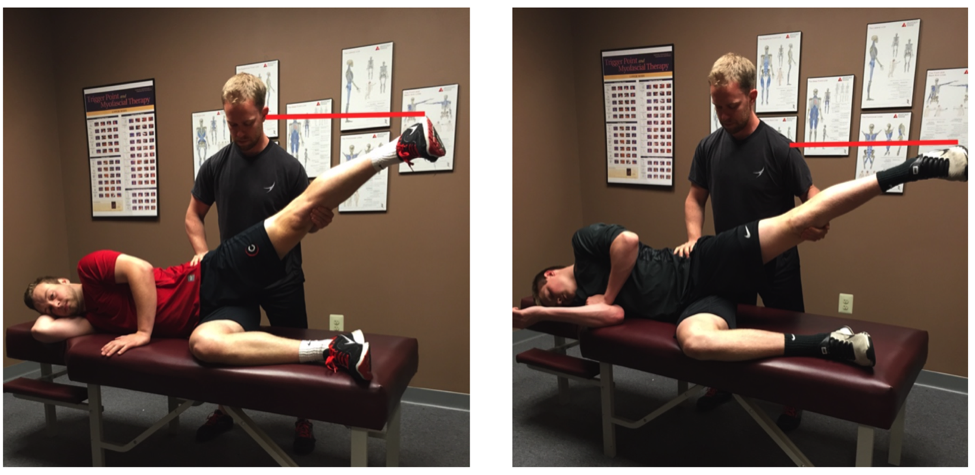
Another way to illustrate this is to consider the lateral split.
The further apart the feet spread, or the further the hips move into this abduction position, the lower the hips drop. So if someone doesn’t possess the hip mobility in this direction, they’ll have to stand up higher to allow for a full stride.
This, along with a lack of ankle mobility, is one of the major reasons players will adopt a higher skating position. Again, all of this just illustrates that mobility in very specific areas can improve skating position, stride length, power through push-off, and ultimately speed. In other words, mobility work IS speed training, and if a player with a mobility restriction just runs more sprints, they’ll be missing out on a huge opportunity to improve their speed.
Note how greater hip abduction range of motion allows the player in red to achieve a much lower hip position, despite being several inches taller than the player in gray.
3. Muscle Size/Strength
Within a similar context, one of the major limitations to skating speed, particularly in high school and younger aged players, is a lack of lower body strength. Strength is a function of both how large the muscles are, listed as “muscle size” on the chart, and how effectively the brain can activate those muscles to produce force.
Strength can limit skating speed in two important ways.
First, if a player doesn’t possess the strength and local muscular endurance, listed in the stamina column, to maintain a low skating position, they’ll start to stand up taller as fatigue sets in. As they stand up taller, their skating stride shortens, they produce less push-off force with each stride, and they slow down.
Secondly, speed is largely determined by how much force a player can put into the ice with each stride. The more force that pushes into the ice, the further the player is propelled forward. By improving the player’s ability to produce high levels of force, you allow them to increase their propulsion with each stride, which simply means that each stride will push them further forward, allowing them to cover more ice with the same number of strides. Force is really just another way of saying strength. So in this way, strength training is really speed training.
Great example of a player possessing significant relative strength in a single-leg pattern.
4. Rate of Force Development
Lastly, ROFD stands for rate of force development. If a player produces the same amount of force, but does it faster, it will shorten the time it takes for them to complete the stride, allowing them to initiate their next stride sooner.
I don’t see this a lot, but in some players that have spent a lot of time developing strength using traditional bodybuilding or powerlifting methods, they’re capable of producing high levels of force, but they do so slowly, so the thing that’s limiting their speed the most is their ability to produce that force at a faster rate.
This is really the first time in this discussion where sprinting, plyometrics, and other more traditional speed and power work has a place in improving a limiting factor to speed.
That isn’t to say that these methods aren’t important in a comprehensive speed development program, but hopefully you now have a better appreciation for how speed training is MUCH more than just simply running.
Relevant Tests for Tracking Progress
There are a lot of performance tests available to help provide insight into limiting factors to speed development, and many of them have merit. Below are a few that I’ve found particularly effective, both in terms of the information they provide and the ease of implementation.
Mobility/Stability
This section could easily be its own article, but in the interest of simplicity, players should have some assessment of ankle mobility, hip range of motion, and single-leg stability. I’ve used several tests over the years to accomplish this, but want to highlight the Y-Balance Test, which has a few notable benefits:
Performance in this test correlates with ankle dorsiflexion and hip flexion range of motion, two important areas for achieving an optimal skating depth
The test serves as a reasonable off-ice assessment of stride length
Some studies have found a relationship between performance in this test and injury risk
The Y-Balance Test is really designed to be an end-range stability assessment, but if you watch how the player goes through it closely, you can get a sense of what may be limiting them from going further. For example, if the knee doesn’t smoothly drift forward over the toes without the heel popping up, the player may have an ankle mobility restriction.
Addressing mobility restrictions and improving single-leg stability should improve performance in this test AND stride length on the ice.
Speed/Acceleration
20-Yard Sprint with 10-Yard Split Time: The body positions, movement pattern, and ground contact time in the first few strides of acceleration more closely resemble the characteristics of skating than top-speed running.
With this in mind, a 10-yard sprint provides valuable information about a player’s ability to accelerate.
However, because hockey players aren’t the most polished sprinters (and they don’t need to be, as mentioned above), there can be a lot of variability in the start. Extending the sprint 20-yards gives a great indication of the players early and late phase acceleration while minimizing the impact a variable start will have on the overall time.
Lower Body Power
Vertical Jump: The vertical jump is one of the most commonly used tests to assess lower body power, and has been shown to moderately correlate to on-ice sprinting speed.
Aside from published research studies, I’ve personally been involved with testing a wide range of players both on and off the ice (youth players, junior teams, NHL Development Camps, NHL Training Camps, Olympic Training Camps, etc.) and the relationship between VJ height and on-ice speed is consistent across all of these groups, making it a suitable option for all players.
Part of the value of the test is that it’s so heavily used that it’s fairly easy to find normative data to look at how a given player compares to others in his or her age group, playing level, etc.
Equipment can be a limitation for some, so using a broad jump (or long jump) is a reasonable alternative. However, I’ve found that broad jump distance correlates with height, so ideally you’d divide the jump distance by height to get a scaled number to track over time.
Lateral Bound: This is a movement included in most hockey training programs, but not one many players are using to track progress.
Compared to the vertical and broad jump, this tests power in a lateral/horizontal pattern, which is more specific to skating, and provides an opportunity to identify side to side imbalances. I’ve also found that in players that are quick on the ice, but don’t have great vertical jumps, they tend to perform well in this test. Including both tests gives a more complete picture of the power profile of the player.
Leg length also plays into jump distance in this test, so it’s important to take a quick measurement of that (or split distance) as well.
I’ve published normative data for players in different age groups here: Hockey Power Testing.
Lower Body Strength
Dumbbell Reverse Lunge (5-RM): For strength testing, it’s possible to get a really good snapshot of the player’s ability to produce force through their lower body with this test.
Similar to the lateral bound, the reverse lunge is a unilateral exercise requiring single-leg stability and dissociated movement between the two legs, two fundamental characteristics of skating. It’s also a fairly easy movement to teach, so it’s safe to implement with players across all age groups.
Strength will fluctuate across developmental years, but by the time players hit high school, they should be able to use at least their body weight in external load (e.g. 90lb dumbbells for a 180lb player).
Wrap Up
There are two major points I want to leave you with.
First, developing speed involves a lot more than running sprints. It’s important to recognize the potential limiting factors to a player developing and expressing higher levels of speed to ensure these are being addressed through a comprehensive training program.
Second, running through these (or similar) tests can be helpful in both identifying individual areas for improvement and ensuring that a player’s training program is leading to the desired results.
The ability to produce force is the foundation for producing force quickly, the recipe for speed. If a player does not have adequate strength, that should be the primary focus. If the player is very strong, but doesn’t perform well in the jumping or sprinting tests, then exercises to improve rate of force development and acceleration should be the primary focus.
A well-designed, comprehensive speed training program should lead to improvements in all of these areas. Addressing a player’s limiting factors is the key to optimizing his or her speed development.
This is a no-brainer if you happen to work with hockey players.
What’s refreshing about this resource is that, while Kevin works with NHL players and has worked with many elite level hockey players throughout his coaching career, this is about keeping things simple and honing in on the basics.
This is about making better athletes.
Speed Training for Hockey is currently on sale at a hefty discount for the next two weeks, so act quickly before the price jumps up.
I had a new client start at CORE recently who, before we even met in person, let it be known that 1) he hated techno and 2) he hated squats.
Well, why don’t you let me know how you really feel?
Personally, whenever I email someone for the first time, my approach is to just, you know, introduce myself, say I’m a big fan, and maybe butter them up with a savory compliment like “oh, and your cat’s adorable.”
I generally refrain from taking a proverbial shit on the things the person on the other end enjoys:
“…and while I’m at it, Tony, I also hate 8o’s cartoons, cheese, rainbows, and your kid.”
I’m exaggerating of course, but once I dug a little deeper and had a bit more back and forth with this individual I got a better sense of his lack of enthusiasm towards squatting.2
When “Ken” came in for his initial assessment he noted that he had, at one point, enjoyed squatting.
Admittedly, those days were more than a decade ago, and despite his current disdain for all things squatting, he was still very much interested in putting them back into his training repertoire and giving them a go again.
The obvious question from me was, “why?”
“If you don’t like back squatting and more to the point, they hurt, why insist on doing them? We can also perform other variations – Goblet, Front, Zercher – that may be a little more back friendly.”
“That’s the thing,” he said, “they didn’t always hurt. When I trained all through college and into my early 30s I never had any issues.”
“But then, you know, I became more sedentary due to life, was stubborn and not taking into consideration I wasn’t 25 anymore, and things just fell apart.”
SIDE NOTE: “Ken” is 47, works long hours mostly at a desk, and I can’t stress this enough, hates techno…;o)
To speed things up all I’ll say is that, while Ken isn’t the most supple person in the world, nothing during his initial assessment came up as a stern red flag or required an exorcism. Sure, he had a few aches and pains, but nothing outside of the normal “niggles” that come with the territory of lifting heavy things for a large portion of one’s life.
I did notice with his passive vs. active squat screen that his active ROM was limited (while his passive ROM was pretty darn okay).
Pertinent information. And if you want to know why that’s pertinent information read the article hyperlinked a sentence above this one.
He also noted he had worked with several trainers in the past who, like me, noticed his lack of ROM with his active squat.
Seriously, read the article.
It’ll help.
As a result he was used to being given a laundry list of hip mobility drills in addition to a plethora of aggressive soft tissue “smashes” to perform daily:
A1. Take a 88 lb barbell and roll it over your thighs. Have someone stand on it and jump up and down for added pressure. Doesn’t that feel great!?
A2. Take a lacrosse ball and poke around in your glutes. If you feel nothing, glue on some razor blades to make it more challenging. Splendid!
A3. If neither of those work, go get a chainsaw. RELEASE.
brb
Moreover, Ken was also given poor advice and told to arch his lower back aggressively whenever he squatted because, #powerlifting.
As a result, whenever he hit a certain depth – usually juuuuust as he passed 90 degrees of hip flexion – he’d compensate with more lumbar flexion and exhibit what’s often referred to as “butt wink.”
Photo Credit: GirlsGoneStrong.com
Again, pertinent information.
No wonder his back always hurt when he squatted:
His issue wasn’t a mobility issue, but rather a POSITIONING issue.
Squat cues that work for powerlifters usually don’t work well with non-powerlifters.
Alignment Affects ROM
To be clear: I am not some anti-anterior pelvic tilt lobbyist.
Anterior pelvic tilt is normal.
There’s a natural lordotic curve to the lumbar spine which is accompanied with a slight forward/anterior tilt of the pelvis.
It’s when it becomes excessive – or people are encouraged to seek it out – that it can (not always) elicit negative repercussions.
Ross et al (2014) noted that:
In 3D modeling of pelvic motion from x-rays of test subjects an increase of anterior pelvic tilt of 10 degrees resulted in:
In short: more anterior tilt (may) require more spinal motion during squatting exercises compared to more posterior tilt.
The dotted section(s) to the left represent the acetabulum (or hip socket). As you move down from A to C we lose site of the acetabulum due to increased anterior pelvic tilt. This will incite increased bone on bone contact – or impingement – sooner as we go deeper into a squat.
Now, I am not suggesting we all walk around in more posterior pelvic tilt like a bunch of Ed Grimley wannabes:
However, what I am suggesting is that nudging a little more posterior pelvic tilt so our clients/athletes get out of their aggressive anterior pelvic tilt (and closer to neutral) may be the more appropriate long-term play.
Sure, it may entail “some” releasing of this and “some” mobilizing of that…but not as much as most people think.
Much of the time the more pertinent approach is to have your clients adopt a better bracing strategy in addition to spending more time strengthening the anterior core and glutes (both of which aid in posterior pelvic tilt).
Likewise, I don’t feel cuing people to “arch their lower back” during a squat is beneficial. As pointed out above, increased anterior pelvic tilt resulted in increased impingement of the hip. Once someone runs out of room in his or her’s hips, in order to squat deeper they have to gain ROM elsewhere.
Their soul lower back.
Moreover, the reason many powerlifters adopt a hard arch when they squat is more out of necessity than because it’s better.
They wear gear/squat suits (that require an aggressive arch in order to hit passable depth).
Photo Credit: EliteFTS.com
People who don’t compete, don’t wear squat suits (and “passable” depth is arbitrary and highly individual anyway).
Circling back to Ken (remember him?), all I had him do in our initial session(s) was to appreciate POSITION. I took away the cue to arch his lower back, and instead had him focus more on posteriorly tilting his pelvis to scoot him closer to neutral (which, remember, is STILL an anterior tilted position).
He was able to squat pain free AND was able to squat deeper without “falling” into that butt wink posture.
It’s been a bit, but Part III of Kevin Mullins’ “Corrective Exercise” series is finally here.
I’d sorta mirrors the anticipation everyone had for the Game of Thrones season premiere this past week, except not even close.
Sorry Kev: dragons will always reign supreme over ankle dorsiflexion…;o)
NOTE: Stressing the word “finally” above had nothing to do with Kevin actually writing the article (which he submitted weeks ago), but everything to do with ME and my nincompoopness in actually publishing it.
You are a fitness professional who wants to train people – AKA provide them with enough of a fitness stimulus to generate the results they’ve paid you for. You also want to help them overcome pain and dysfunction in their body.
Thankfully, this series of blogs have got you covered and smothered like Waffle House hash browns.
Which brings us to the final piece of the puzzle – corrective exercises for the knee and ankle.
Many people who would consider personal training deal with some level of knee or ankle problems. In fact, it could be argued that everyone walking around this beautiful Earth has dealt with knee or ankle pain/dysfunction at some point in their lives.
(Tony raises hand. I spent the better part of two years in the early 2000’s working around a cranky left knee.)
A proper discussion of these two joints, one mobile and one stable, would not be complete without a discussion about the role of the hips and feet in the function and performance of the knee and ankle. Our feet are our first and only contact with the ground during much of our lives. Any disruption of their optimal function is going to send dysfunction up the kinetic chain into the ankles and knees.
Just the same, the hip, and its multitude of muscle attachments, functions, and movement possibilities can have a dramatic impact on knee function. Tight hip flexors or imbalanced anterior/posterior chain development can change how the patella tracks over the feet – a recipe for pain or less than desirable movement outcomes. As a proud fitness professional, you should be capable of assessing, correcting, and training clients past many of the common problems that might land on your doorstep.
In this post we’ll explore the anatomy and physiology at play when knees and ankles are the weakness in someone’s kinesiology. We’ll discuss the interplay between the hip-knee-ankle-foot. Then, like the other articles, we’ll discuss five specific issues that most trainers encounter and show off a few new exercises that you can use today.
And then we’ll tie a fancy bow on this corrective series, gather all our jackets and move towards the exits. I hope you’ve found a friend
Basic Knee and Ankle Anatomy – Skeletal
(nerds only)
When looking at the knee joint, we are only considering four specific skeletal structures:
The Femur – the longest bone in the human body is also our primary weight bearing skeletal structure. The femur’s entire function occurs at the hip. It can move through flexion and extension, abduction and adduction, external rotation and internal rotation, and circumduction.
The Tibia and Fibula – load bearing bones of the lower leg. Their design allows for weight transfer in gait and for optimal loading of the lower body during any exercise that creates knee flexion or extension.
The Patella – a bone unlike most others in the body, the patella is interwoven with the tendons that cross the knee joint and serves as a cover for those tendons. The structure of the patella also improves the mechanical efficiency of these tendons.
The ankle joint is a bit more complex though. We must consider the bones of the foot to some degree.
The Tibia – The load bearing bone from earlier is also a major contributor to ankle function. The medial malleolus, a bony growth on the inside of your ankle is located on the tibia. At the ankle, the medial malleolus plays a role in ankle eversion and inversion.
The Fibula – Like the tibia, the fibula is a load bearing bone that also functions during ankle eversion and inversion. It’s bony process, the lateral malleolus, is located on the outside of the ankle.
The Talus – a unique bone in a variety of ways, the talus serves as the base for the tibia and fibula to plant upon. Both dorsiflexion and plantar flexion involve the talus changing position in relation to the rest of the foot. The talus also plays a role in eversion and inversion.
The Calcaneus – connected to the talus via the subtalar joint – the calcaneus functions as a base of support for the structures above it. It hosts insertion points for a variety of muscles and tendons – most notably the Achilles tendon. It is the largest bone of the foot.
(Foot) Metatarsal – critical bone structures that connect the toes (phalanges) to the larger structures of the foot. The metatarsals are critical for weight transfer and distribution and while they don’t move like other bones in the body – their ability to adjust to pressure is critical for elite performance.
(Foot) Phalanges – the toes are the final element of this puzzle. Understanding that the toes can and should flex and extend as a result of ground force reaction or conscious neural action is critical to optimizing the foot’s function. While there may never be a “toe day” – we need to train the function of the phalanges to ensure their relationship with the other foot bones, the ankle joint, and even the knee and hip, are optimal.
Basic Anatomy of the Knee and Ankle – Muscular
It is important to discern the muscles that act on the knee and the ones that act on the hip.
Sure, both are in the thigh and run the length of the femur. However, since the knee joint is designed for flexion and extension – we are only considering the muscles that do just that. With that said, realize that the muscles that do function at the hip must do so properly. Otherwise, the knee joint will act to compensate for dysfunction at the hip and that will cause a host of problems too.
The following addresses strict flexion and extension of the knee joint.
The primary flexors of the knee are:
The muscles of the hamstrings (biceps femoris, semitendinosus, semimembranosus)
The gastrocnemius, popliteus, gracilis, and sartorius are synergistic muscles
The primary extensors of the knee are:
The muscles of the quadriceps (rectus femoris, vastus lateralis, vastus intermedius, vastus medialis)
Now, when looking at the ankle we find simplicity and complexity at the same time. On one hand, there are a bunch of muscles that control the toes and ankle joint that aren’t needed in the typical fitness professional’s vocabulary. Simply put, most trainers don’t need to know the minor details of how the fibularis brevis functions, or where the insertion point of the flexor hallucis longus is.
But they need to know they exist.
(Although, more knowledge is never bad and anyone with an interest in self-myofascial release therapy should understand the interplay between these lesser known tissues).
We do need to know that ankle and foot function relies on many more players than just the prime movers. We do need to understand that dysfunction at the ankle could be a myriad of things and not just a blanket statement about someone’s gastrocnemius.
So, we will address the for major movements of the ankle and point out the muscles for each.
** Take note of just how many more plantar flexors there are compared to dorsi flexors. This could explain why we are so strong with our “calf-raise” exercises and why we typically can access a greater range of plantar flexion under control than we could with dorsi flexion. **
Primary Movers of Eversion
Fibularis and extensor digitorum longus
Primary Movers of Inversion
Tibialis anterior and posterior
When looking at this from a slightly higher viewpoint – we see that we have significantly more muscularity driving both flexions of our ankle joint. The lack of muscularity controlling eversion and inversion explains why we don’t load up on an exercise that challenges that motion. Moreover, it probably explains why “rolling” an ankle can be so devastating – we have so little musculature to control that motion.
Going a little broader, we see that muscles of the lower leg have multiple functions. The tibialis anterior dorsi flexes and inverts the foot while the tibialis posterior contributes to plantar flexion and inversion. The extensor digitorum longus everts the foot while contributing to dorsi flexion. These functions are not accidental – they are essential evolutions and developments of our anatomy to meet the demands of our life.
If we are to succeed in our experience as human beings, then we must be able to communicate with the ground effectively. Thus, the muscles that control our foot, ankle, and knee become our first point of contact with outside world.
Understanding their function, their interplay, and their contribution to elite performance is critical to maximizing the impact you’ll have on your clients and your purpose as a coach.
Basic Movement Physiology
The function of the knee and ankle are highly dependent upon the task we are trying to perform and whether the hips are involved.
For example, the knee will flex and extend during traditional deadlift, but not at the same degree that they would during a front squat. The same logic also applies to the amount of dorsiflexion needed from the ankles to meet that demand.
A different example points to our running stride.
The gait pattern that most elite distance runners take involve very minimal action at the ankles and toes. This sort of “hammer-foot” stride is highly efficient and puts the emphasis on the hips and knees to generate all forward locomotion. Sprinters, however, require maximum action from all the joints of the foot and ankle in order to increase velocity and compete successfully.
Thus, understanding physiology of these structures requires an understanding that optimal function is dependent upon the demands of the task.
Still though, a few notable things exist:
1. When the ankle is in full eversion or inversion – there can be an issue with one’s ability to flex and extend the knee. This is because of the change in position of the inferior aspects of the tibia and fibula creating an up-chain manipulation in their superior aspects (which form the knee joint). It is minor in most but could explain why individuals who live in eversion or inversion find discomfort in their knees.
2. Triple-Flexion (hip, knee, and dorsi-flexion) is the most loaded position of the body because of the major muscles that have created force (tension). In most populations, the greatest power will come from individuals in this position. The stacking of joints lowers the center-of-mass and improves the ability to generate tension.
3. Triple-Extension (hip, knee, and plantar-flexion) is the “tallest” the structures of the lower body will get. The process of going from triple-flexion to triple-extension typically generates the greatest joint velocities.
4. The running stride requires a rhythm between hip-knee-ankle-toe action. Upon foot strike, the toes should flex, which drive the ankle joint into plantar-flexion, assist in driving knee extension, and hip extension. The cycling leg does the exact opposite as it returns to the pre-strike position.
The Major Issues
The knee and ankle joints can be seriously injured during sports and accidents in life. None of the issues discussed below involve torn ligaments, broken bones, or even severe tendonitis. The conditions listed are ones that routinely plague clients who are either inactive or too active with poor function.
In fact, many of the issues of the knee come from overuse of the joint without proper interaction with the hip and ankle. Runners and lifters alike may experience knee pain when their form is off. Likewise, many untrained or detrained individuals deal with knee and ankle dysfunction as a result of their sedentary lifestyles.
And don’t forget about footwear.
There is a cost and benefit to each type of footwear that you and your clients are wearing.
Dress Shoes and Boots – great for making a suit look dapper, or kicking tail on a job site, but atrocious for allowing mobility in the foot. Basically, you feel like you are walking inside of bricks.
High heels – an entire day spent into plantar flexion is not good for anyone. Spending additional time walking in them can hurt the wearer’s ability to distribute their weight once they are out of the heels. Great calves though.
Flip Flops – If you are wearing these, then you are probably at the beach. Sweet. However, that sliding and gliding motion that you are using to keep them on is wreaking havoc on your ankle function while also driving too much knee extension.
O-Lifting Shoes – Having your heels elevated when driving your heavy squats or cleans is awesome – can you say performance? However, if you spend most of your day in these shoes than you can bet your bottom that you’ll begin to lose optimal ankle function since you aren’t feeling the ground.
With all of that said, let’s focus on the five most common things you’ll see in your clients and discuss exactly what is going on.
Lack of Dorsi-Flexion
A lot of people struggle to dorsi flex their ankle in response to loading. In fact, a lot of great coaches, including Tony, have pointed out the importance of adequate dorsi flexion for someone to succeed in a squat pattern.
High quality athletes and desk jockeys can both suffer from this issue. It isn’t simply limited to an inactive or undertrained population. It must be dealt with though if someone is going to optimize the function of their hip-knee-ankle and drive greater results in their programs.
Strengthening the muscles that drive dorsi-flexion while also “stretching” the ankle into these positions with bands or straps is usually the best intervention. We aim to increase mobility, improve strength and stability, and begin providing context and practice with traditional strength training movements such as the squat or lunge.
Runner’s Knee (Patellofemoral Pain Syndrome)
A sort of unofficial name, runner’s knee refers to the over-development of the quadriceps (knee extensors) while also keeping the hamstrings (knee flexors) and glutes underdeveloped. In addition, tightness and exhaustion of the plantar flexors can lead to instability and pain at the knee joint.
In fact, there is some evidence out there that shows that some runners experience a mild shift of their patella in space. Only a few millimeters – this shift can cause significant pain and contribute to the official name of the condition (patellofemoral pain syndrome).
The training for individuals presenting this issue is quite simple:
Release and relax the muscles that plantar flex the ankle and extend the knee.
Strengthen and tighten the muscles that dorsi flex the ankle and flex the knee.
Train the glutes to improve hip drive in the running stride
Traditional strength training and myofascial release typically take care of the problem, although a cessation of running in the short term is almost always a good idea.
Knee Valgus
One of the most misunderstood dysfunctions of “the knee” is a hip issue. Many trainers can coach “knees out” until they’re blue in the face and still get no change in the performance of their client.
First, knee valgus refers to the inability of the hip abductors and external rotators to fire appropriately, thus causing a collapse once tension reaches a certain threshold (such as the bottom of a squat).
Image Credit: prehabguys.com
Now, sometimes this only requires good coaching as the client or athlete simply doesn’t know they are doing it or that isn’t ideal that they are doing it.
We must be wise though. Coaching knees out could be driving excess ankle inversion, which changes the relationship of the tibia/fibula with the knee and could lead to torque being experienced in the knee joint as the body seeks to overcorrect the inversion. This isn’t a common worry – but it is possible.
The training cure though will involve strengthening the abductors and adductors of the hip to improve knee tracking in a variety of exercises. It is important to keep in mind that overtraining the abductors can lead to other problems that only arise when the adductors are forgotten about.
There could also be something going on at the ankle too…
Inappropriate Eversion and Inversion
This one sounds a little silly, doesn’t it?
Inappropriate sounds like someone left their pants at home.
But it points out a deficiency that a lot of people have. Whether it be from a lack of coaching and training, or the development of patterns by accident through sport and training – many people lack the right ankle position to complete the task they are attempting.
Think of that client that can’t stop squatting without eversion. Every repetition pushes them into their toes and insole (often leading to valgus). It could be coaching (or a lack thereof), it could be muscle weakness, or it could be a neural disconnect between their brain and their ankles (they don’t know they are doing it).
Just the same, there are people who can’t seem to run on their big toe. They’ll stride flat footed, especially on the outside of their heels, and wonder why they aren’t getting any better at running. These people have not unlocked enough plantar flexion or awareness of their inversion.
It is exceptionally common to see in long distance runners.
Having the wrong ankle position is coachable and trainable. You must relax what is overused and overworked and strengthen what is left behind. There will be specific protocol for whatever you are seeing. Simply look back at the muscular anatomy and select exercises and interventions that are appropriate.
Disconnect of Hips from Knee/Ankle Function
The final issue that people have with their knees and ankles is that they have no idea they have a pelvis. It is as if they believe their lumbar spine connects to the back of their legs…
No really, you probably have a client or twelve who seem to have no idea how to flex and extend the hips. As a result, everything hurts their knees and ankles. Squatting hurts, running leaves them achy, and they absolutely despise lunges.
They aren’t broken thankfully.
They just need to discover their glutes.
They need to learn how to flex and extend the hip with a lot of exercises that leave the knees out of it. So, deadlifts, hip thrust, banded abductions, Copenhagen side planks, and some anterior core work will do wonders to wake up their hips, stabilize their core, and allow them to excel and knee-dominant and gait patterns. Want to learn more about this? Check out my last installment on the hips.
The Exercises
1. Bulgarian Split Squat to Ankle Glide
https://www.youtube.com/watch?v=2WO3-DQenTI
Your goal with this bodyweight exercise is to create a crossover effect between knee flexion and dorsi flexion. By working with the single leg variation – you’ll enhance your clients focus on one specific ankle while simultaneously exposing them to pause reps for the single leg squat variation. You can train them and correct them at the same time.
2. Banded Dorsi to Heel Raise
https://www.youtube.com/watch?v=qrMjjZKkQ8Y
Great for runners and athletes, but effective for everyone, this ankle exercise only requires a band and a seat.
The goal here is to maximize both dorsi flexion and plantar flexion in the same movement cycle. This sort of training allows for you keep the muscles that control both actions in relative balance. This is not unlike being on a calf raise machine and allowing your heels to dip below the step.
3. Barbell Hip Thrust w/ Banded Abduction
One day I want to call Bret Contreras and thank him for his research on the glutes. (Although this video is of Ben Bruno – a stud coach in LA who does NOT like burpees). Discovering that the hip thrust provides more activity of the glute muscles than other exercises is critical for the development of aesthetic and athletic glutes.
Adding in the abduction component at the top is a sure-fire way to ensure your “knees-out” coaching cue for valgus hits home. The band ensures they move from the hip joint instead of just torqueing at the knees. Add in the isometric hold of the glutes and you’ll be sure to work the hip component of knee stability.
4. Duck Walks
https://www.youtube.com/watch?v=beIn56rJGmU
This is an absolute torture device. Duck Walks, loaded or unloaded, drive the body into that triple-flexion position we discussed earlier in the blog. This coiled position strengthens the posterior chain and improves dorsi-flexion by keeping our feet in a set position.
A highly integrated exercise – the duck walk can be used for neural prep or as a burn out after your primary work is done. Sure, its goofy and it doesn’t “seem” like it is going to do your body any favors, but try it and feel how your systems work together to hold isometric tension.
5. Reverse Nordic Curl to Nordic Curl Superset
https://www.youtube.com/watch?v=H-WpX-dnBuY
We want the quadriceps and hamstrings to be in relative balance for optimal knee function. Depending on our choice of sports or training – one may overpower the other a little. That discrepancy though shouldn’t be a chasm.
Hitting both versions of the Nordic curl in a single superset provides an opportunity to train the muscles in a unique way using only bodyweight.
BONUS: Sprinting
https://www.youtube.com/watch?v=3YqQum4emVw
The act of sprinting is one of the most athletic things the human body can do. The whole body must get in on the act if we are to excel.
Specifically, for the knee and ankle, sprinting helps drive a low-level of eversion while demanding quality cycles through plantar flexion and (mild) dorsi flexion and knee flexion and extension. Add in the function at the hip and we’ve found the perfect lower body exercise for improving someone’s function and interplay between these regions.
Obviously, not every client could sprint or should sprint. Be wise with your prescriptions and coach who you are with, not who you wish they were.
Finding the Exit
So, once again we conclude that we can intervene in our client’s discomfort and dysfunction with exercises that not only correct issues, balance muscles, and improve coordination, but also drive a fitness stimulus.
The knee and ankle are interesting joints in a sense that they have less muscle mass around them than the hips and shoulders. But that doesn’t make them any less important. In fact, their proximity to the ground – a constant in our lives – makes them more important than most trainers think. Everything that is dysfunctional at the foot, ankle, and knee will run up the chain into the hips and spine and even the shoulders.
Help your clients discover their foot stability, ankle mobility, and knee stability and you’ll help them discover a better body – both in performance and in aesthetics.
Thank You
Thank you for your time.
Thank you to Tony for allowing me to share my ideas on his website – a treasured space on the internet.
Whether you visit him for his pop culture references, his biceps veins, or his absurd level of knowledge about the body – you’ve made a great choice.
I truly hope you have learned something from this series and enjoy my writing style. I poured a lot into this, and into my book, Day by Day. I hope I can download everything I have learned (good and bad) from me to you every chance I get.
Like I say to my clients, “let’s get just a little bit better every day.”
Check Out Kevin’s Shit
You can read more of Kevin’s stuff at his website HERE.
In the last article – HERE – we looked at how we would address the issues that occur at the shoulders and thoracic spine. We discovered that optimal shoulder function comes from a healthy scapulohumeral rhythm, a mobile thoracic spine and humerus, and strong scapula and core muscles. In the end we identified common problems and proposed unique exercise solutions that can not only correct issues when they arise, but also strengthen the capacity of the joint altogether.
That followed my opening article in which I discussed my stance on the current state of our industry and how we’ve gone overkill in regard to corrective exercises. You can read that HERE.
Which brings us here to the next installment of the series – a similar dive into the lower back and hip joint, an anatomically different, but physiologically similar region of the body.
You’ll discover how lower back pain isn’t simply the lower back, how hip dysfunction or immobility requires more than flexibility and blood flow, and that integrated three-dimensional movements are the key to unlocking the hips and core.
As Shakira sings, “hips don’t lie”.
We are going to dive into the anatomy of the region, the physiology of the segments, and biomechanical implications that must be considered by any professional worth their salt.
We are going to unlock our, and our client’s, potential by adding another five great exercises to the equation too. But first, I want to take a moment to clear the air and amend a point I made in my previous post.
An Amendment on the FMS
In my last article I made a bit of a blunder when I described an issue that I have with the Functional Movement Screen. In my efforts to write a short, and interesting, piece of literature that covers a complex topic I did not effectively communicate my viewpoint on the matter. My claim that “the FMS puts the fear of God into trainers” isn’t quite accurate.
Brett Jones of FMS and I had a call on the matter and enjoyed an outstanding conversation on the FMS, how trainers are using it, and my specific area of concern.
Brett Jones (Note From TG: NEVER make Brett angry. Ever. Just kidding. Brett’s as professional as they come and one of THE best presenters I have ever had the pleasure of learning from. But seriously, don’t feed him past midnight.
He drew to my attention that the FMS, when taught properly and used properly, especially after the level 2 certification, provides trainers a lot of tools to correct and address issues that are present in the screens.
And he is spot on.
In my experience with the Functional Movement Screen, and the literature it publishes, I’ve found tremendous success in identifying, addressing, and correcting flawed patterns. The tools are present for a trainer to succeed.
So, to that end – the FMS itself is not an issue, and in fact, the certifications and resources that Gray (Cook) and Lee (Burton) provide are high on my list of recommended education for trainers. Simply put, much of the responsibility lays on the trainer performing the assessment to ensure they understand what they are screen, why they are doing it, and what it all means regarding the client’s exercise program.
And so, my point is really this:
“The FMS can put the fear of God in trainers who haven’t invested enough time to understand its purpose and nuance. This can be avoided by investing in your education and diving head first into new information.”
Basic Hip and Lower Back Anatomy – Skeletal
When looking at the skeletal anatomy of the spine and hip we find that it is quite simple. There are four major considerations:
The thoracic spine – capable of flexion, extension, and rotation. In an ideal world the thoracic spine handles the bulk or rotation and extension of the spine.
The lumbar spine – capable of flexion, extension, and rotation. In an ideal world the lumbar spine serves more as a stable base for movement that allows the pelvis to move underneath, and the thoracic spine to move above.
The pelvis – capable of anterior tilting (pouring water out of our belly button), posterior tilting (pouring water out of our back) and lateral tilts to either side (pouring water out of our sides).
The femurs – capable of internal and external rotation, flexion and extension, as well as abduction and adduction. Each of these movements are necessary to generate the variety of locomotion patterns we execute daily and for the specific movements we perform in training.
The ankle and foot are also capable of impacting health of the hips too, especially in the running community. Issues in these lower joints can cause negative effects to move upwards in the kinetic chain and begin causing negative adaptations in the hip joint or lumbar spine. We will address these correctives in the final part of this series, Hip-Knee-Ankle-Foot, so stay tuned.
For now, simply acknowledging their role in the process is enough.
Under the same principles, the shoulders can also impact the function of the hips. A dysfunction in the shoulders, such as upper cross syndrome, impacts the T-spine, which disrupts the lumbar spine and pelvis. Improving the health of the shoulder joint can help alleviate the poor postures that stress the lumbar spine and allow for a better functioning pelvis that experiences the ranges of tilt patterns because the lack of tightness in the lower spine. The scapula specifically should be considered (and will be in our correctives).
Basic Anatomy of Spine and Hips – Muscular
There are muscles that could be mentioned in this section that run very deep in the body and have very specific function.
The multifidus for example is a muscle that runs along the spine and has an important function; yet, our training practices aren’t exactly targeting it.
It is always good to know these types of muscles, such as the quadratus lumborum, obterus group, gemelli4 , and the aforementioned multifidus. Still though, this article is meant for our day-to-day efforts and most trainers simply don’t need to consider these things
There are some major players that you need to know though:
The abdominal wall, specifically the transverse abdominus, rectus abdominus, internal and external obliques, and psoas muscles. These muscles flex, extend, and rotate the spine and some act on the hip as flexors.
The gluteus maximum, minimus, and medius. These muscles act on the hip as external rotators and hip extensors.
The four muscles of the quadriceps, three muscles of the hamstrings, the tensor fascia latae as well as your abductors and adductors all act on the hip and knee joint. These muscles drive motion of the femur in the hip socket in a variety of ways that are unique to each pattern. In the next section we’ll isolate the specific motions and what muscles are involved for bookkeeping purposes.
The erector spinae, the quadratus lumborum, lattisimus dorsi, and lower trapezius muscles function on the thoracic and lumbar spine from the posterior of the body. These muscles are critical for putting the T-spine in the right place and stabilizing the L-spine during movement.
Basic Movement Physiology
Knowing what is in play is only half of the battle.
Note From TG:Goddamit Kevin. Rule #239 of being a nerd is that whenever the phrase “only half the battle” is used it must always be followed with GOOOO, Joe
In fact, knowing the structures and muscles involved is irrelevant if we don’t understand how they create movement in the body. To avoid blowing this article out into a thirty-thousand-word book on physiology we are going to have a down and dirty list of functions and the muscles that do the work.
I implore you to read and learn more about the muscular physiology that drives these movements from other resources. Play with things at the gym and try to “feel” what you can. I felt obligated to include this information in an honest effort to create the best free guide to hip correctives you’ll find. What you do with your education from there now rests in your hands.
Spinal Rotation or Lateral Flexion – Any of the core muscles mentioned above when functioning unilaterally. If one side of the rectus abdominus fires, then you’ll see lateral flexion and some rotation. Other rotators include the internal and external obliques and serratus anterior.
Hip Flexion – psoas major, iliacus, rectus femoris, sartorius, tensor fasciae latae, adductor longus and brevis, gracilis, pectineus. Some fibers of the glute minimus and medius engage here.
Hip Extension – glute maximus, biceps femoris, semitendinosus, semimembranosus. Some fibers of the glute medius engage too.
Hip Abduction – the glute maximus, minimus, and medius as well as the tensor fasciae latae. The piriformis functions when the hip is at 90 degrees.
Hip Adduction – adductor longus, brevis, magnus, pectinius and gracilis
Hip Internal Rotation – tensor fasciae latae, adductor longus, brevis, and magnus, pectineus, sections of glute medius and minimus
Hip External Rotation – piriformis, gemellus superior and inferior, obturator internus and externus, glute maximus, minimus, medius, psoas major, sartorius, quadratus femori
Now, I realize that this list reads like the appendix of a textbook, but don’t get lost in the noise. Notice the tremendous amount of overlap. You’ll see that the glutes have multiple functions as do the adductors and the TFL.
This sort of information at least shows us what the major players are going to be.
The Fascial Integration
We must also give attention to the intricate layers of fascia that are found in the core, hip, and thigh. Whether we address it through myofascial release or integrated non-linear movements, we must give it attention.
As noted in the previous edition, fascia is a highly communicative tissue that can arrange our body and its structures at a speed that is closer to the speed of light or sound than it is the speed of our cognition.
Fascia adapts, positively or negatively, to the stress placed upon it. Sit in a chair all day? Well, your fascia is likely bound up and dehydrated. Exist in a world where yoga, integrated movements, and sports are a major focus? Chances are you have healthy fascia.
The utilization of non-linear movements is one of the best ways of to improve fascia.
The Major Issues
The issues that occur at the spine and hips are almost always interconnected. A client could deal with just one or all of them.
Chances are that you’ll deal with all of these issues in some point in your career.
It is important to read and learn each of these as their own issue while also understanding that a client could show up to you with a Royal Flush of dysfunction. Luckily, the correctives we’ll discuss at the end are Swiss army knives – they are great for everyone.
1) Desk Posture
Once again, our lovely desk posture makes an appearance on the list. It is important to acknowledge the impact that upper cross syndrome (UCS) can have on core function, and thus hip function. If someone is slouched over with internally rotated shoulders, a kyphotic thoracic spine, and weak abdominal muscles, then we can very likely ascertain that their hips aren’t going to function optimally.
The lack of thoracic extension, poor function of the core muscles, and the overextension of the erector spinae and trapezius muscles dramatically impact the way someone can function up and down the length of their spine.
Ironically, many of these same flaws are also present in lower cross syndrome (LCS), which involves the muscles of the lumbar spine, abdominal wall, and the hips. Dysfunction caused from sitting all day can make the muscles involved weak (glutes and abdominals) or tight (muscles of the lower back and the hip flexors).
When a client presents these issues, especially together, it can be hard to prescribe any challenging exercises because their entire torso is locked from neck to butt. It is important to spot these issues early and begin implementing a corrective strategy that gets that client on the right path.
Thankfully, we’ll have some exercises below that will be great for both UCS and LCS issues.
2) Excess Anterior Tilt
When the pelvis is stuck in its “tipped forward” position for too long there are issues that can present themselves at rest and during exercise. In fact, continuing to exercise, especially with exercises that promote even more tilt, can cause damage to the vertebral discs.
In this position the erector spinae and QL are pulled tight while the anterior core is left in a lengthened and overstretched state. This sort of weakness in the abdominal wall makes optimal hip function harder to achieve and can lead to injuries at the spine.
Another unfortunate consequence is the overextension of the spine, or flaring of the rib cage, which can create the appearance of a midsection that is holding excess bodyfat. This bulge is simply a result of poor posture and would disappear once the pelvis is set back to neutral.
It should be noted that though that the pelvis should be able to anterior tilt through a full range of motion – it just shouldn’t be stuck that way.
3) Excess Posterior Tilt
The exact opposite of anterior tilt is the posterior version, which is when the pelvis is tilted back too far. This “belt-buckle to nose” condition is often found in individuals with lower cross issues since their abdominal walls are weak and their hip flexors overactive.
This position pulls the glutes completely in line with the body and flattens out the lumbar spine by ridding of the natural curvature of that region. This is not only “less attractive” due to the appearance of having no ass, but it also dangerous to load someone who can not achieve even low levels of hip extension and hip flexion. When someone is stuck here – they effectively have no idea of how to move their hips.
The corrective strategy here requires specific interventions that improve the awareness of the client as well as the strength of the glutes, hamstrings, abdominal wall, and even latissimus dorsi muscles. Additional efforts can be spent to improve external rotation of the femur and abduction too.
Once again, the hip should be able to posterior tilt during some movements and to help create stability.
4) Sticky Femurs (no, this isn’t technical)
One of my favorite terms for someone lacking the ability to rotate their femurs in their hip sockets (internally or externally) is “sticky femurs.” What I mean by this statement is nothing more than the image of having gum stuck in the joint that prevents optimal movement.
This is a combination of a lack of mobility in the joint due to not experiencing enough movement variation. Very active people could have “sticky” hips if they don’t cross train or experience movements in all three planes. Many “big” lifters struggle with external and internal rotation at the hip.
The other side of the coin is weak external or internal rotators that are incapable of owning the position that we put the femur in with excellent mobility. This is very common in dancers, those who practice yoga, or others who don’t actively strengthen these muscles. Detrained individuals fall into this category too. The mobility is there, but strength at end ranges is not.
5) Poor Coordination
Sometimes the issue is simply getting people to start exercising more and feeling their body move in a variety of ways. Frequent exercise, especially when done with coordination as the end goal, can improve a lot of functions of the hips on its own. It is amazing just how bad things can get when someone is rusty or de-conditioned.
Of course, you’ll need to spend time mobilizing and strengthening the various elements of the hip joint, but you’ll likely see increased output by simply exposing clients to new forms of movement and exercise. Any training program that features unilateral, contralateral, ipsilateral, and bilateral movements in all three planes is ideal.
6) Weak Core
Lastly, poor strength in the core itself can cause serious issues. It can derail any segment of the body since the primary function of the core itself is force transduction – AKA – translate forces from the limbs to each other and to the external environment.
A strong core is capable of remaining stable as the limbs create and accepts force. We must ensure our clients can move through all three planes of motion, with optimal function at the joints, with a variety of loads and challenges, because they possess a strong core. For this reason, most of our programming for the core should emphasize creating, and maintaining, tension.
The Corrective Exercises
Once we dive into the corrective strategies it is important to acknowledge that all these movements can be used to help with each issue. All these movements in some way will impact the ability of the client to succeed in overcoming hip dysfunction.
Each are also excellent in isolation as warmups, isolated correctives, and “fillers” between primary movements (as Tony often discusses). The Sumo deadlift, obviously, is a primary movement that should occur early in a program, especially if we are loading it up.
1. Glute Bridge Pullovers
https://www.youtube.com/watch?v=744uVr_qbqM
This simple variation of the traditional glute bridge accomplishes two major things:
Drives all the major benefits of the traditional glute bridge
Incorporates lat tension into the glute bridge – a key point for deadlifts and squats
You can strengthen the lats, glutes and abdominals while also addressing coordination issues. This exercise can help with every problem listed above except for “sticky femurs.”
2. Foot Elevated Glute Bridges
https://www.youtube.com/watch?v=uB_OanZw_Js
Another glute bridge variation that can dramatically improve the strength of the hip muscles (both flexors and extensors). By elevating the feet, you can increase the range of motion you’ll experience and improve your ability to drive into the bridge.
The key is to manage the lumbar spine and avoid overextension. The sort of exercise is great for strengthening the core, improving pelvic tilt issues, addressing coordination, and improving posture.
3. Cossack Squats
https://www.youtube.com/watch?v=XC0InYzYb00
A highly advanced variation of a lateral squat – the Cossack squat asks for an incredible amount of external rotation from the femurs. It targets the muscles that drive abduction and hip flexion and extension while moving through the frontal plane.
You can use your arms to help counterweight your body as you go down and find depth. Ease into the motion and look to improve your depth and mobility over time. This is an advanced exercise that can be regressed to holding onto something like a squat rack to help with weight transfer.
4. Copenhagen Side Planks
For some reason we love naming exercises after places – this side plank variation being no different. However, this is one of the most incredible ways of working the adductor grouping without needing to add external load. You’ll also integrate your internal rotators and the muscles of the rotary core. This sort of combo lends itself to improving strength and coordination.
Your goal should be to squeeze the bottom leg towards the bottom of the bench without rolling over and dumping the tension in the side plank.
Drive yourself to maintain an ideal side plank posture the entire time.
5. Loaded Marching Carries
https://www.youtube.com/watch?v=JuHCDH1T43E
Loaded carries are a movement pattern all their own. Few things can rival the simple effectiveness of grabbing heavy weights and walking around with great posture. This variation though, greatly improves the function of the hips by incorporation intentional hip flexion through the march.
Focus on driving the knees perfectly vertical, play with your speeds, and always emphasize a tight upper back, strong core, and depression of the scapula.
This exercise addresses every single problem mentioned above.
6. Sumo Stance Deadlifts
https://www.youtube.com/watch?v=XhxviMQEWOM
The validity of a medicine is always in its dose. Sumo stance deadlifts are one of the best corrective exercises you could program assuming:
You or your client are ready for the stress of loaded hinges
You choose the appropriate version for where you are in your training routine
You have earned the right to be here by exercising pain free with less aggressive modalities.
The reason that the sumo stance is so great is that you are literally working all of the muscles of the thigh, hip, core, and upper back at the same time. The external rotation and abduction of the femurs improves the strength of the muscles involved while also helping clients discover new mobility and neuromuscular coordination. This pattern is especially useful for those who spend most of their days sitting.
7. Loaded Beast to World’s Greatest Hip Opener
https://www.youtube.com/watch?v=spt_l-XhZRE
An interesting cross between a traditional mobility exercise and one of the loading phases in Animal Flow – this is one of my go to exercises for increasing the dynamic ability of my clients.
This version allows you to go fast or slow depending upon skill set while also loading the hips through a full flexion and extension cycle, improving coordination, and integrating the upper body and lower body together in a mobility movement.
You can use this as a “energy system” filler if you so choose (and your client is ready).
BONUS:
8. Hinge Position Face Pull
https://www.youtube.com/watch?v=JibVKRxbgAs
A lot of clients need help discovering how to hinge. Those same clients also struggle with maintaining tension in their cores and lats too. This exercise combines an active movement of the shoulders (great for shoulder health) with a passive hip hinge to improve core and hip strength.
Add this into any of your programs as a variation of the face pull that challenges your clients do more than just yank on the cable.
Wrapping it Up
Your ability to improve your client’s function around their hips depends on your ability to address the mobility and stability needs of the segment while also ensuring they are getting enough of a training stimulus to cause change. Understanding the nuances of the anatomy and physiology is a critical step in developing progressive programs that correct issues and cause a training effect.
The final part of the series will discuss the relationship of the hip-knee-and ankle.
I’ve often championed the notion that there’s “no such thing as textbook technique.”
How we’re taught to execute certain exercises in a textbook often won’t translate to the real world because, well, we don’t live in textbooks.
This is a theme that’s hit on several times in The Complete Trainers’ Toolbox. Sam Spinelli, one of the contributors, was kind enough to share a bit of an amuse bouche from his presentation “All Things Squats, Knees, and Hips” with everyone today.
To check out the full presentation, as well as contributions from eight other renowned industry leaders, go HERE for more information.
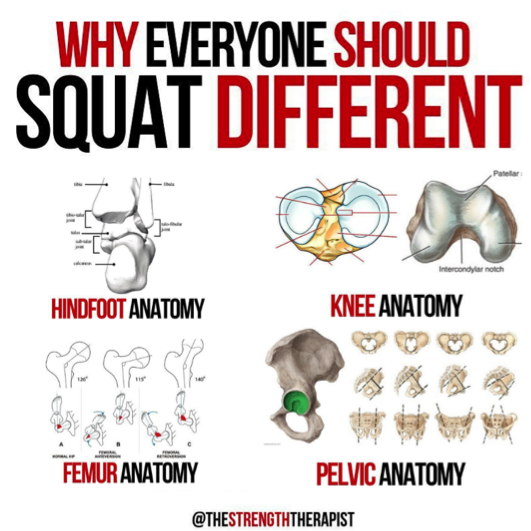
Humans are these incredibly awesome, adaptable, and diverse creatures.
Within our awesomeness, over time we have adapted to have a diverse set of unique features in our anatomy that provides for a wide range of movement from person to person. This is something that we did not readily acknowledge for a long time and tried to fit people into square holes.
The squat is a perfect example of this topic.
For such a long time it has been advocated to squat with your toes forward and perfectly hip width apart. The unfortunate thing is that this limits a significant majority of people from being able to squat comfortably – or to an appreciable depth.
While some people may be able to do so with practice and working on range of motion, for a vast majority it is just not realistic due to their bony anatomy.
As we examine the ankle, knee, and hip, we can see that there is significant variation within the bones forming them and the resulting joints.
For example, at the hip we have an acetabulum that can vary in depth of which will impact how much motion a set sized femoral head can have. This will impact the capacity of motion for hip range between individuals, leading to diverse squat stances already. When we begin to layer on the other ways our anatomy differs, it compounds and leads to a breadth of variations in how people may squat.
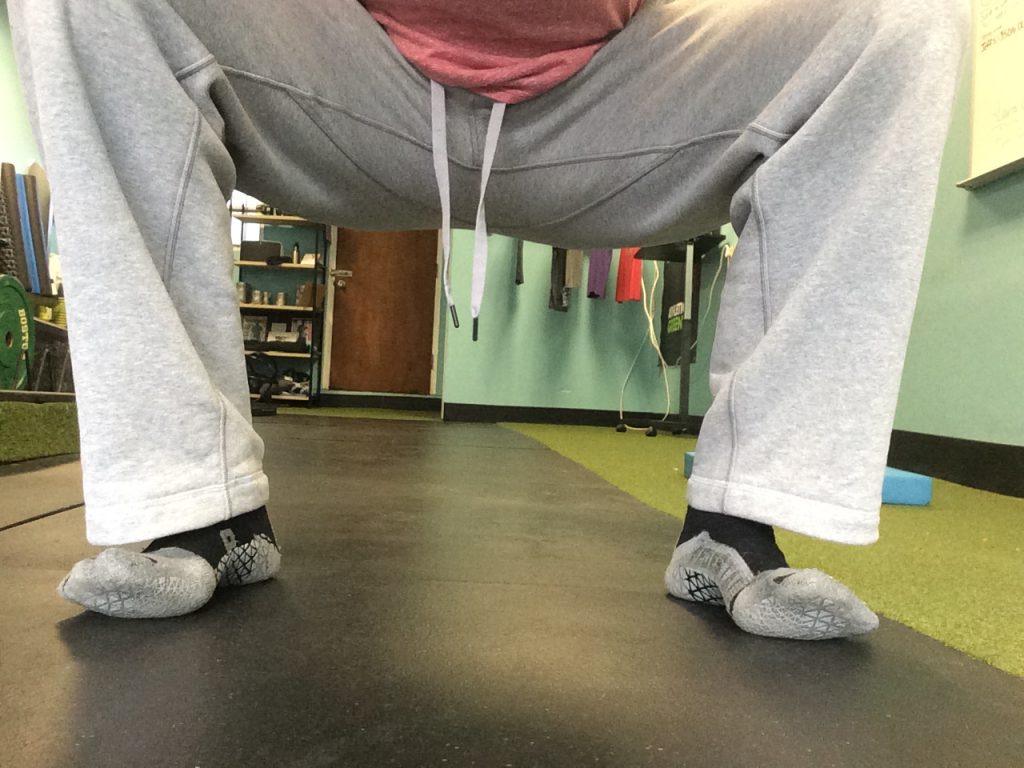
How Should I Squat Then?
There isn’t a set stance that will accommodate everyone – some people will do well with a hip width stance and slight toe out, others may do better with a narrower stance and feet directly forward. Finding what works best for you can be a challenge at first and require some experimentation.
To help expedite the process, try out these four methods:
1) Find Your Squat Stance – Standing
2) Find Your Squat Stance – Supported
3) Find Your Squat Stance – Seated
4) Find Your Squat Stance – Kneeling
The goal with each is to start with feet together and progress foot/knee width. You will find that one width generally feels better than the others, that’s the one to stick with for now. Then you can start playing around with foot/knee angle and continue experimenting.
This will get you a great head start on your squat stance and making it unique to you.
Two additional details – you may find your stance more comfortable with your feet not symmetrical and you may find that your stance changes with time. These things are normal for many people.
Did I Just Blow Your Mind?
This is just the tip of the iceberg in terms of stuff I cover in my presentation “All Things Squats, Knees, and Hips” in the Complete Trainers’ Toolbox, an online resource that became available this week that also features presentations from eight other industry professionals – including Tony Gentilcore, Dean Somerset, Dr. Lisa Lewis, Alex Kraszewski, Kellie Davis, Meghan Callaway, Dr. Sarah Duvall, and Luke Worthington..
It includes 17 total hours of content covering a wide range of topics every health/fitness professional is bound to relate with. It’s on sale this week at a significant discount, but only until Sunday, February 17th at midnight.
Excellent strength coach, and outstanding Canadian, Dean Somerset once stated in an internet post, or maybe it was a blog, “there is always a cost of doing business.” He meant it as a point of emphasis when talking about the various effects of training programs and specific exercises. But he also could have extrapolated it outwards to reflect the stresses of our daily lives.
Poor posture while seated for twelve hours is going to have a cost associated with it just as German volume training.
Note From TG: OMG, German Volume Training brings back the worst memories. I don’t know which was worse: getting kicked on the balls or GVT?
For this reason, the fitness industry has made a major shift towards corrective exercises. Once seen as the tools of progressive physical therapists – these mobility, stability, and integrated exercises have become critical elements in training programs for elite athletes, nimble geriatrics, and the average Joe and Jane alike.
The growth of corrective modalities in conventional personal training is a good thing overall. However, as I pointed out in the introduction to this article series – HERE – there exists a very big downside to the obsession with movement perfection and body correction.
There needs to be a better way of correcting people’s movement flaws, overcoming their specific weaknesses, and getting them to a place where they can safely train hard. Far too many coaches are “under-training” their clients because they are investing too much time “correcting” things. At some point we need to get people training hard towards their actual goals.
Using Your Head For Their Shoulders
There may be no part of the body more susceptible to under-training than the shoulders. With multiple skeletal structures, a bunch of muscle attachments, and a relationship with the spine – there are a lot of reasons that someone wouldn’t be “allowed” to train hard with their shoulders.
Training them includes more than the traditional bodybuilding approach too.
The glenohumeral joint is involved in all upper body pushing and pulling motions as well as the specific isolation exercises that are popular in bodybuilding programs (such as lateral raises or chest flyes). The scapula and clavicle are too, but their positioning on the body also impacts movement such as the deadlift and squat.
Because of their high level of integration with every exercise we do, the shoulders are often the most banged up part of a client’s body. Our poor postures and ill-advised training programs aren’t helping us. Often the two compound each other and only worsen any dysfunction that exists.
Hence the need for correctives.
Really though, the shoulder itself is a bit of a miracle joint – with all the muscles that cross it, the fascia, the nerves, blood vessels, and obvious skeletal structures – it is amazing that it functions as well as it does.
But there can be a whole host of issues going on, or there can be just one. And that is what is most challenging about assessing and correcting shoulder dysfunctions.
It could be as simple as improving someone’s ability to retract and depress their scapula, such as when someone’s posture isn’t where we’d like it.
Or as complex as improving external rotation of the humerus while also stealing more extension from the thoracic spine and stability from the scapula during upward rotation and elevation, such as when a client wants to get better at pull-ups.
No matter how intense the problem is it is important that we as coaches keep our processes simple.
Removing the Restrictions
Yet, simple is not how most coaches approach shoulder health.
In fact, if you were to follow many of the conventional prescriptions that are floated through the industry, then you’d avoid many of the things that produce big results for your clients in favor of small correctives that make small changes. While some clients do need more intervention with these corrective methods – most simply need enough to create an opportunity for more intense training.
If you were to follow many of the guidelines that accompany something as notable as the Functional Movement Screen (the FMS), then many of your clients would not be allowed to press, or pull vertically, or load up abduction or adduction in the frontal or transverse planes until they were able to get a “2” on the shoulder mobility assessment.
While Gray Cook and Lee Burton did an incredible job creating a screening tool that helps coaches discover dysfunction and lack of movement prowess – they also created a system that is preventing a lot of clients from actually getting better.
Note From TG: For anyone interested (I.e., everyone) I wrote about my experience taking the FMS and what I took from it HERE.
The protective measures and governing principles of systems put the fear of God in personal trainers who use them. Many are afraid of loading anything until they see a two on the scoreboard. It is a steady dose of low intensity or no intensity correctives until that day.
Which is where the problem with corrective exercises starts:
Low to no intensity corrective exercises aren’t why clients improve over time. Instead, it is the strengthening exercises that come after these correctives that matter most.
If we are to improve how we utilize corrective exercises in our programs, then we must be willing to accept that what we now know isn’t perfect. We must be willing to entertain the idea that there is a better way of doing business. It is this exact mentality that drives innovation in technology.
It will drive innovation in fitness if we let it.
—-
(It is important to pause here and make a statement – this article is not meant to treat, diagnose, or prescribe methods or modalities for someone who is dealing with diagnosed injury or dysfunction in their shoulders. Traumatic injuries, conditions such as frozen shoulder, cervical kyphosis, and others require a finer touch from qualified medical professionals.)
If Not This, Then What?
Corrective exercises are like the bore that drills tunnels in the side of a mountain. They create the space for the construction to take place, but they aren’t the construction. You wouldn’t want to drive through a tunnel that hasn’t been reinforced with steel supports and millions of pounds of concrete, so why do you think that corrective exercises are enough to create a finished product in fitness?
The mobility and stability exercises that we define as “correctives” simply create the space for more optimal change to take place. They create the opportunity for well-selected strength exercises to change the tissues for the better.
For shoulder health we find that the classic approach of wall-angels, thoracic roll-overs, and cat-cows are simply creating the opening for which exercises like loaded carries, supinated pulldowns, and banded retractions fill with strength and stability. Our goal needs to be to do enough to get to the exercises that stimulate adaptation and create positive change; in the shoulders and in the rest of the client’s body.
Our responsibility as trainers is to help our clients overcome dysfunctions and improve their movement quality – sure. But our job also implies that we help our clients burn calories, build muscle, and come just short of conquering the universe.
Before diving into the actual corrective exercises that will open the gates for us to train with the intensity our client’s want and need, let’s ensure that everyone reading is on the same page on the anatomy and physiology of the shoulder joint.
The Basic Anatomy and Physiology – Skeletal
When looking at the shoulder joint you are presented with three major bones: the clavicle, the scapula, and the humerus.
The clavicle (or collarbone) is the most stationary of all of these structures, but its lateral aspect does elevate and depress in reaction to movements of the other bones. The humerus, the upper arm bone, is designed for external and internal rotation within the socket – known as the glenohumeral joint.
The humerus can move through flexion, extension, abduction and adduction, and horizontal abduction and adduction by rotating around the glenohumeral joint in each of the three planes (sagittal, frontal, transverse). These movements are aided by the function of the scapula.
The scapula (or shoulder blade) is the large bone in the back of the body. It is capable of six motions: elevation, depression, upward rotation, downward rotation, protraction, and retraction. These movements are also correlated to the three planes of motion too – sagittal, frontal, and transverse respectively.
The spine is also involved in shoulder mobility and stability is often left out when looking at function. We will explore this relationship in the next section when we begin looking at how core function can impact shoulder mobility as well as how thoracic extension is necessary for optimal function of the shoulder joint.
The Basic Anatomy and Physiology – Muscular
The human shoulder functions as incredibly as it does because of the incredible number of muscles that are involved. Some control the humerus, others control the scapula, and others control the spine.
Most of these muscles are found in the back.
When looking at the muscles that contract at the shoulder, we must separate the muscles that control the external rotation and internal rotation of the humerus from the muscles that create the six motions of the scapula. While some muscles share functions – it is important to identify its primary action and what it acts upon in order to better understand how the shoulder wants to function.
The four muscles of the rotator cuff are most responsible for the external and internal rotation capacity of the humerus.
There is evidence to support that the triceps are involved in external rotation, especially under load (just turn your arm around as far as you can right now, and you’ll feel the lateral head of the triceps contract). Therefore, the triceps join the supraspinatus, infraspinatus, and teres minor as external rotators of the humerus.
With that claim we can also ascertain that the biceps and pectoralis group are involved to some degree in internal rotation (although there is significantly less IR available at the shoulder joint). The subscapularis is the internal rotator of the cuff.
When examining the muscles that move the scapula, we are simply looking at the muscles of the upper back; the lats, teres major, rhomboids, trapezius, levator scapulae, the serratus and the three external rotators of the cuff. Each of these muscles have specific functions on pieces of paper, but it is imperative as coaches that we realize that most exercises performed in a gym setting involve more than just one of these muscles doing one of these functions.
It is easy to point at the traps and say “oh, they are elevators and contribute to upward rotation.” It is less easy being able to look at a flawed motion and know exactly what is wrong:
For example, many coaches will point at someone having issues with retraction and think “ah, the upper traps are overactive and the teres major/minor need strengthening.” They could be right and probably are in a population of people who sit with rounded thoracic spines and internally rotated shoulders.
Add in forward neck and shrugged shoulders and this “diagnosis” seems spot on.
However, getting just the teres group to fire without activating the infraspinatus or supraspinatus is nearly impossible in a traditional training setting. Getting someone to stay out of their upper traps sounds like a great coaching cue, but that requires getting them to fire the muscles that contribute to scapular depression; the lower traps, pectoralis minor, and latissimus dorsi at the same time – something most clients (or you) can’t do consciously.
In fact, a lot of scapular depression comes from the ability to put the thoracic spine into extension. Doing so involves activation the lowest fibers of the traps, the lats, the upper abdominals, and a whole host of muscles that are so deep and connected to the individual vertebrae that considering them in training is pointless.
When these muscles contract and thoracic extension takes place, you find that the scapula better slide into the depressed position.
The Core Connection
Yet, thoracic control isn’t completely isolated either.
It is very hard to contract the thoracic muscles without some level of core control. In this instance, the core includes the anterior muscles of the core that we know (rectus and transverse abdominals, internal and external obliques, and Psoas Major.
It also includes the muscles of the posterior core: the quadratus lumborum and the erector spinae.
Conscious contraction of these muscles allows for the core to hold tension, which better stabilizes the lumbar spine, which better allows the thoracic spine to go into extension, which better allows the scapula to depress, which better allows the humerus to externally rotate. As you can see, everything is connected, which is why we can’t use such generic correctives to solve complex problems.
A Less Important Factor?
You’ll notice that we haven’t yet mentioned the deltoid – the most known shoulder muscle. For all the attention it gets in bodybuilding circles its function is not as critical to shoulder function as you’d believe. The anterior fibers assist in internal rotation and drive flexion of the arm while the posterior fibers aid in external rotation and initiate horizontal abduction. The lateral fibers function to create abduction of the arm in the frontal plane.
From a corrective standpoint, it is very rarely an issue with the deltoid that proves to be the problem. In fact, it is often the overdevelopment of the deltoids and upper traps and underdevelopment of the rotator cuff muscles that create impingement issues in dedicated lifters. Great corrective exercises keep the deltoids involved and avoid shutting them out.
The Hidden Gem
In recent years we’ve come to learn that the fascia in our bodies is more than just a covering and more than just extra tissue that gets cut through in surgery. It is a living tissue that is involved in our function on a day by day and minute by minute basis.
In fact, research from Michol Dalcourt and the team at the Institute of Motion have proven that the fascia can communicate information across the body faster than any muscle tissue. Its ability to compress and expand is crucial for athletic development.
Unfortunately, many fitness professionals see it as tissue that is addressed with foam rollers, lacrosse balls, and other release methods. This isn’t wrong of course as these implements can do well to increase blood flow, increase hydration of the fascia, and improve mobility of the joint in question. However, we can also train our fascia just as we train our muscles. We must look to incorporate the variety of slings that Thomas Meyer’s discusses in his text Anatomy Trains.
In our solutions section we’ll explore a few ways to do that to improve the function of the shoulders and truly correct any issues that exist.
But first, we must identify a few of the most common problems.
Common Problems
1) Desk Posture (UCS)
The most common problem that a client will present in regard to their shoulder health is the classic “desk posture”. The scapula sits in protraction and elevation while the humerus’ are internally rotated. This posture is held for eight, ten, and twelve hours a day. Over time the pectoralis muscles get tighter, the trapezius muscles lengthen, the muscles of the scapula and glenohumeral joint get weaker, and the client continues to worsen.
The most advanced form of this condition is known as Upper Cross Syndrome (UCS) – a severe condition of immobility that usually involves additional intervention with physical therapists, and sometimes, orthopedic surgeons. This posture often presents forward neck as a well – a dangerous condition of the cervical spine.
The treatment for individuals in this position is to correct their posture and work to move them in better retraction, depression, and external rotation. However, many of the common methods do not provide enough intensity to stimulate muscle growth or strength adaptations in the muscles of the upper back. It is crucial for trainers to invest time in building their clients upper backs and coaching optimal patterns if the corrective interventions are ever going to stick.
2) Poor Scapulohumeral rhythm
For many people the pain they experience in their pressing and pulling motions is a result of a poor pattern being present. Of course, there are others who have legitimate issues such as shoulder impingements, strained muscles of the rotator cuff, or overactive trapezius muscles that make doing certain movements nearly impossible. The rest though, simply need help reworking their patterns and an emphasis on strengthening the muscles that control those patterns.
The scapulohumeral rhythm refers to the quality of movement that occurs when we consider the scapula and glenohumeral joints interaction. People with great rhythms typically an exercise pain-free while people who lack control and patterning struggle to accomplish even the most basic tasks.
This topic is quite deep, but in short realize there is a relationship between the position of the humerus and where the scapula “should” be.
For example, in a traditional dumbbell overhead press the scapula should be upwardly rotating and elevating as the humerus adducts towards the midline at the top of the press. Many people will execute their press and have little to no movement out of their scapula, thus causing increased stress on tissues that shouldn’t need to encounter them.
3) Lack of External Rotation
One of the issues many clients face is the inability to rotate their humerus back. This is more than just the presence of too much internal rotation (such as with U.C.S.). The muscles responsible for external rotation of the shoulder are powerful muscles that also engage in the motions of the scapula. Lacking strength in these tissues can cause someone to become more internally rotated, but also makes it incredibly hard to achieve external rotation at the glenohumeral joint.
This matters for more than just mobility.
Popular exercises such as pull-ups require a person to own a certain amount of external rotation in order to execute the motion. So too does the overhead press. Lacking the ability to achieve optimal end range of E.R. makes both movements, and so many others, hard to accomplish.
It is important to understand that the exercises we use to improve external rotation put the humerus in a greater rotation than we would normally encounter in traditional lifting. But, this sort of work is necessary to strengthen and stimulate the muscles that create E.R. and maintain it in an isometric contraction (such as during a overhead press).
4) Weak Core and Poor Thoracic Extension
As stated earlier, the core and spine play a major role in whether the shoulders function optimally. A lot of lifters never develop optimal shoulder health because they create mobility by overextending their lumbar and thoracic spine to compensate. This is especially prevalent in ego lifters performing an overhead press with a massive amount of “layback”.
Lacking the ability to contract the anterior core and stabilize the lumbar spine makes it significantly harder for someone to master true thoracic extension. The ability to lift the ribs and extend the thoracic spine allows for better depression, retraction, and downward rotation of the scapula. These motions are direct opposites of the posture that many fall into as a result of upper cross syndrome or “desk posture”.
Strengthen the abdominal wall and muscles of the T-spine is imperative to optimizing shoulder function. Much like the foundation of a skyscraper must be firm and set underneath the construction, so too does our core and spine for our shoulders.
5) Weak Upper Back and Lack of Awareness
In a lot of cases, especially in individuals who do not regularly engage in an exercise plan, there is simply a lack of proprioception and strength in the muscles that control the scapula and glenohumeral joint. Often, there is nothing “wrong” with this population other than their lack of sensory awareness and force production capabilities.
Clients like this require more exposure to well-coached patterns and a progressively overloaded strength program that allows their muscles to adapt over time. It may be beneficial to use low intensity correctives to prime a specific pattern and create mobility in the joint prior to loading the muscles with traditional methods.
It is critical that we stop seeing all clients as wrecked when they are unable to perform a specific task. For many people, especially with something as obscure as the FMS, it is simply an unfamiliarity with their body and the demand you are placing upon them. Increase their exposure to well-coached exercise instead of trying to fix something that isn’t broken.
New Solutions
As we dive into the specific movements it is important for us to realize that these are just a few examples of great movements that can be used to strengthen and stabilize the shoulder joint. Some of these movements are common and others are painfully boring (in a sense that we aren’t shaking the Earth).
However, simplicity is often the fasted route to success.
A few of these movements are going to be outside the realm of normality for some coaches. Many traditional strength coaches would look at Animal Flow as a weird form of yoga and dancing, but it is that arena that brings the fascia into the fold. Other movements are simply manipulations of variables in the training arena, such as the angled press, that most people aren’t considering.
1) Dual Kneeling Band Pull Apart
https://www.youtube.com/watch?v=3rrHNDcVa9s
The band pull apart is nothing new.
However, adding in the kneeling position asks us to contract our core and our glutes – two major parts of our foundation. In doing so we can better extend our thoracic spine, which in turn allows for better retraction of the scapula.
2.1) The Full-House (2 Cables/3 Motions)
https://www.youtube.com/watch?v=COSRT7nPTPc
This multi-pattern movement asks for retraction of the scapula, then retraction into downward rotation and depression (with external rotation of the humerus). Lastly, the overhead press asks for elevation, upward rotation, and forces the external rotators to fire hard to prevent the arms from collapsing forward of the line of gravity.
This sort of movement is incredible for grooving the scapulohumeral rhythm, improving upper back strength, and increasing external rotation of the humerus. It is quite the challenge and needs to be done extra light. Five pounds was the resistance in the videos.
2.2) Second View
https://www.youtube.com/watch?v=Qt8ex9TL8GQ
3) External Rotated T, Y
https://www.youtube.com/watch?v=3Juj1iYiJFE
A simple variation of traditional T and Y – this a movement that can be used to improve retraction of the scapula while strengthening the external rotators. It forces the trainee to own their humeral position and originate movement from the glenohumeral joint while remaining set onto stable scapula.
This exercise also promotes additional thoracic extension.
4) Angled Press
https://www.youtube.com/watch?v=FVPsVXWXds0
Far too many people contraindicate the overhead push pattern when someone is dealing with shoulder dysfunction. If we were to listen to the FMS, no one who can’t get a two on the shoulder mobility exam should ever press overhead. Yet, tons of people can press pain-free without getting a two.
This exercise helps bridge the gap between overhead pressing and not. The slight angle (about 15 degrees) allows you to load up the deltoids a bit without creating a perfect opposition to gravity. The neutral grip, forward elbow, and emphasis on tempo allows us to focus on scapulohumeral rhythm. Use this as a primary exercise after preparing clients for their workouts. This will correct a lot of flaws so long as the movement remains pain free.
5) Supinated Pulldowns
https://www.youtube.com/watch?v=TbIy3pH0nlo
At first glance this looks like a standard, boring pulldown.
Yet, it is the dramatic emphasis on depression and elevation of the scapula that makes this one stand out. Far too many folks get on the pulldown and just start yanking on the bar to get their set done. The motion becomes about completion instead of optimization.
The supinated hand grip helps keep the humerus in a slightly more externally rotated position while also prevented much of the internal rotation that happens with heavy pronated pulldowns. The focus here is to emphasize absolute end ranges. Feel the scapula elevate while maintaining control and then drive them downwards into full depression at the bottom.
6) Simple Animal Flow (Beast Hold to Scorpion to Alternating Crab Reaches)
https://www.youtube.com/watch?v=x27wT-nxUkg
A lot of you will look at this and wonder – why in the heck am I going to do all that flailing? Yet, animal flow is an incredible discipline that emphasizes loading of a lot of our passive structures – the fascia, the connective tissue, the skeletal system. Strengthening these things is imperative to the absolute realization of healthy shoulders. Specifically, the external rotation of the humerus in set crab position is a great tool to have in your arsenal.
7) BONUS: New Way to do Chest Flyes
https://www.youtube.com/watch?v=hcRTVz4aWOE
Lastly, I want to share the new best way for you to execute chest flyes.
See, the chest flye is one of the most favorite exercises in bodybuilding culture. It causes a tremendous stretch of the pec fibers and can help the person doing them build the muscle they crave. Yet, there is a ridiculous amount of sheering force placed upon the shoulder joint when the dumbbells reach the bottom of a traditional flye.
So, instead of using dumbbells and pissing off your shoulders – integrate this band only variation. The key is to press out into the band for the entirety of the movement, thus keeping a high level of tension on the working muscles without stressing the shoulder joint against gravity. As you fatigue shorten the range and focus on the squeeze.
Putting It All Together
You can correct someone’s shoulders and move their fitness forward at the same time. Your job as a fitness professional is to drive your clients towards the results they want and the results they didn’t know they need. You can still use low intensity correctives in your programs, of course, but it is imperative to go forward understanding that they are simply a very small piece of a much larger puzzle. Your client, if they are to improve, must begin strengthening the muscles by training the appropriate patterns that address shoulder health.
Next: The Lower Back and Pelvis
In the next article we’ll explore the lumbar spine, pelvis, and anterior core and how we can better correct chronic low-level back pain, coach better hinge patterns, and improve our client’s ability to move with confidence.
Two things with regards to the title of today’s post:
I’m thinking it could pass for the title of the next big children’s book.6
Searching stock images for “big toe” pretty much made me want to throw up a little in my mouth. I’d place it somewhere between kipping pull-ups and gonorrhea in terms of stuff I’d rather not see with my eyes ever again.
There’s a lot to consider and that can go awry when discussing the squat. To say there’s a plethora of moving parts – not to mention positional considerations (hand position, stance, bar position, etc) – would be an understatement.
One of the last things you’d probably ever consider when it comes to your squat performance is your big toe. Well, I’m here to tell you that it’s a pretty damn important and something you should consider considering.
Also, this is about as non-pukey of a picture as I could find of a toe.
What inspired this post was an interaction I had with a new client recently. During his initial evaluation I had him show me his squat because he had mentioned the movement has always bothered his lower back.
He’d worked with previous trainers in the past who had attempted to “fix” things, more often than not resulting in him stretching this, smashing that, performing a cornucopia of positional breathing drills while repeating the Elvish alphabet backwards, and otherwise being over corrective exercised to death
In fact, I’d be surprised if I’m not nominated for a Nobel Prize for how revelatory what I did was.
Are you ready?
Wait for it…
Wait for it…
I watched him squat.
https://www.youtube.com/watch?v=a1Y73sPHKxw
I’m flummoxed as to why this seemingly obvious “intervention” is often overlooked. I think a lot of it has to do with something John Rusin spoke about during his keynote talk at the SWIS 2018 Symposium:
“We’re in an industry that gets too distracted by bright, shiny objects.”
Watching someone squat is boring.
Having someone stand in a zero gravity chamber while a bunch of lasers attempt to release their psoas isn’t.
We’ve become infatuated with gadgets and gizmos so much so that it’s become much harder to galvanize the masses into trusting what it is they do best……
………..COACH.
To that point, I’m old school and I just wanted to watch my man squat.
I had him take off his shoes and pants, and it’s here where I noticed something.
I watched his feet and saw that with every repetition his toes would come up off the ground, like so:
FYI: this is a picture of me doing a reenactment. See you in a few weeks at the Oscars.
Now, for the sake of brevity, it is a conversation to have as to whether or not he was cued into lifting his toes off the ground or not? I’ll nip this in the bud and say for the record that he wasn’t.
He was just never coached on how to squat properly.
As such, it became glaringly clear why his back had always been flipping him the middle finger whenever he attempted to squat (Goblet, front, back, all of them).
When your toes – most often the big toe – comes off the ground you lose your core.
Bullet Points (for those of you too lazy to watch):
When toes come up, you lose canister position (ribs stacked on pelvis) and thus lose your core and stability.
When toes comes up, you crank into lower back.
Think more about foot pressure (pushing into floor and even weight distribution on big toe/metatarsal, small toe, AND heel).
Cement toes to the floor.
Take your clients’ shoes off when they squat. It will tell you a lot.
My biceps looks amazing in salmon colored t-shirts.
But Wait Tony, Some Coaches Cue People to Squat With Big Toe Up on the Way Down, and Then to Push It Into the Ground on the Way Up. Are You Saying They’re Assholes?
No.
Coaches such as Mark Cheng and Cal Dietz – who are both the shit – often advocate the big toe stays up on the way down during a squat (but the ball/metatarsal still stays glued to the floor) and then press the toe down on way up.
I find this to be okay – and far be it from me to say they’re wrong. They’re both developing outstanding athletes and making people better.
I just find that with all the other mental gymnastics that come along with the squat – big air, ribs down, sit down, not back, spread the floor, drive your chest into the bar, hips through, don’t poop your pants – that it gets a little crowded when you add in the “toes up on the descent, toes down on the ascent” cue.
As I note in the video above I like to cue the idea of foot pressure – with three points of contact – and to cement the toes down during the squat.
Moreover, the objective is not to grip or dig into the floor with your toes.
“I don’t like “digging” because you don’t want to press the tip of the toe to the ground, more the pad of the toe. Big toe, ball of the foot, 5th metatarsal, heel. Pressing big toe helps the windlass mechanism as well.“
Here’s a nice demonstration of everything in action by Essex, Vermont based strength coach, Jess Voyer (who was kind enough to refer to me as a genius in her IG post. 4,000,000 points to Gryffindor):
Just to help calm the waters: I am not anti “corrective exercise.”
And I am not really going to throw my face into a brick wall.
I respect and can appreciate that, sometimes, our jobs as fitness professionals require us to pump the brakes and to venture down the corrective exercise rabbit hole.
Some people require a bit more TLC with regards to improved movement, motor control, and/or, and I’m paraphrasing here…”just learning to turn shit on.”
Some people will require a laundry list of additional mobility work, stretching, or positional breathing drills to point them in the right direction and to help them feel better.
What I am against, though, and what drives me bonkers, is when coaches and personal trainers go out of their way to:
1) Overstep their scope of practice and end up performing really shitty physical therapy with their clients and athletes.9
OR
2) Highlight every minor “dysfunction” with a client/athlete – excessive anterior pelvic tilt, kyphotic posture, left eye is lower than the right (you freak) – making him or her feel as if they’re walking ball of fail.
Here’s another gleaming example of how TRAINING is corrective and how, if we do our jobs as coaches, we can often accomplish a lot sans the brick wall.
My client, Emily, who’s a trainer herself, has been dealing with some left shoulder issues. I had her come in the other night to see if I could offer some insights and to listen to some sick EDM beats.
The latter has nothing to do with anything, but whatever….give THIS a listen.
Emily showed up and I took the picture below. It shows something clearly awry and that some sort of shoulder clusterfuckey was at play; namely lack of shoulder flexion on the left side.
What was the culprit?
It could have been a few things:
Capsular issue
Lack of scapular rotation (namely upward rotation).
Soft tissue restriction.
Lack of lumbo-pelvic control.
It was a Wednesday.
I don’t know.
What I do know is that I had to respect my lane and understand it wasn’t my job as a strength & conditioning coach to diagnose anything.
I could, however, assess her general movement capacity, use my knowledge of anatomy, and perform a little trial and error to see if I could improve things.
What follows is more or less a brain dump and an attempt to explain my thought process as I worked with Emily for the next hour.
I’m not gonna say that what ended up happening was on par with some Matrix level shit, but I will say I basically know Kung-Fu.
“What actions have to happen at the scapulae in order to get the arms overhead?”
– Upward rotation
– Protraction
– Posterior tilt
Emily wasn’t getting much upward rotation on that left side. When I asked her to bring her arms overhead it was as if her left arm hit a massive speed bump and came to an abrupt stop. She could push through it, but not without pain.
So I had to think about what muscles help with that action (upward rotation)?
– Upper and lower traps
– Serratus
Too, I noticed she also had a more depressed shoulder girdle as a whole; her clavicular angle was more horizontal rather than having a slight upward grade.
HERE‘s Eric Cressey discussing this in a little more detail.
I surmised her UPPER traps needed some attention.
The upper traps often get a bad rap and are avoided like a Coldplay concert. In certain populations (think: desk workers) and instances, the upper traps are OVERactive and can play a role in increased shoulder elevation as well as superior migration of the humeral head, and hence an increased risk for shoulder impingement.
In this scenario, it behooves us to not go out of our way to increase upper trap activation.
However, we often forget the upper traps are a major player in UPWARD ROTATION, not to mention help with scapular elevation…both of which, in my eyes, Emily could have used some more of.I didn’t get over corrective with Emily and start having her perform some voodoo like tapping her pinky finger three times while flossing her teeth with a strain of hair from a Hippogriff.
I didn’t have her perform a laundry list of “correctives” that, for all intents and purposes, would have likely made her feel like a patient and bore her to tears.
Nope, I had her TRAIN and just modified a few things.
We did:
1. Landmine Presses with a Shrug/Reach
2. Face Pulls in an upwardly rotated position (so the upper traps were more engaged)
3. And, instead of performing movements that would pull her into more shoulder depression and downward rotation (deadlifts, farmer carries, etc) we opted for Landmine Squats, Zercher RDLs, and Hip Thrusts.
In short: We turned shit on (upper traps) and trained movements that (likely) wouldn’t feed into the root causes of her symptoms.
Here’s the picture I took at the end of her session:
We’ve all seen the statistic: 80% of the population will experience low back pain in their lifetime.10
Back pain is the single leading cause of disability worldwide. Americans spend upwards of $50 billion per year on back pain. Back pain is the nemesis of all ninjas.
The struggle is real folks.
Given how pandemic the issue is and the sheer number of resources there are on the topic, why is LBP still such a nuisance and the Bane of many people’s existence?11
When it comes to low back pain there is no one clear cut answer or way to explain things. As my good friend David Dellanave would say “different shit is different.”
It’s impossible to definitively point the finger at one or two things and say “there, that’s it. THAT’s why everyone’s back feels like a bag of dicks.”
Certainly we can proselytize, but at the end of the day we’re mostly just guessing at what may be causing someone’s low back pain. We’re using an amalgamation of relevant anecdotes, experiences, expertise, and evidence based research to make those educated guesses.
But it’s guessing nonetheless.
[BEFORE WE MOVE ON: Another good friend, physical therapist Zak Gabor, sent me THIS rather thorough paper on management of low back pain. To quote Zak…”Movement is key, but EDUCATION on false beliefs about the body is arguably most important.”]
A week or so ago as I was watching an episode of VICE News on HBO and one of the main stories that night was on opioid addiction and of a former drug representative who, sadly, because of debilitating low back pain, had become addicted to the very pain killers that had made him so successful years prior.
In the story he described a seemingly endless barrage of treatments ranging from massage therapy and acupuncture to ultrasound treatments, physical therapy, and traction.
It was a hefty list and I can’t remember all of it.
In the end he ended up having back surgery, yet unfortunately was still reliant on pain killers to help with his chronic low back pain.
As the story unfolded they panned to the same individual miniature golfing with his family and I ended up taking a screenshot of him bending over to pick up the ball after sinking a shot.
If I could add sound it would be accompanied with a cacophony of painful grunting akin to a rhinoceros passing a kidney stone.
Now, what follows is not an attempt at me diminishing his experiences, and I’m fully cognizant my only source of info regarding his “treatment” was/is the five minute snap shot I was given from the story.
That said, I wonder how much agony and frustration might have been prevented in his lifetime if someone took the time to show him some basic “spinal hygiene” (to steal a phrase from Dr. Stuart McGill and his book Back Mechanic) tactics to clean up his daily movement?
What might have happened (what can happen?) if, instead of acupuncture, he was shown how to hip hinge well or given a healthy dose of Deadbugs, Birddogs, and Breathing Side Planks?
Repetitive (aberrant) flexion, as shown in the still shot I took, certainly isn’t doing his back any favors. And, I have to assume this type of thing is happening dozens (if not hundreds) of times per day, whether he’s picking up a golf ball or getting out of a chair.
It glaringly demonstrates how we often neglect to address the obvious and simple everyday “hammers” in our lives that can (not always <— this is important) lead to back pain.
I’m talking about the kind of hammers – repetitive movement (repeated spinal flexion, and extension for that matter) – that start off as innocuous nothings (the twist there, the bending over there), yet manifest into something far more nefarious once one’s tissue tolerance is surpassed.13
As my friend and strength coach, Joy Victoria, notes:
“Habitual daily postures and movement strategies have a greater influence, than intentional exercise.”
Massage, ultrasound, etc, while likely part of the puzzle (and can provide immediate, albeit temporary relief), are just band-aids.
I think exercise, and to be more specific, strength, can play an integral role in the grand scheme of things.
However, as fitness professionals it’s imperative we keep a keener eye. Deadlifts don’t cure everything. Recognizing run-of-the-mill wonky movement and attacking that, as trivial as it may seem, can make all the difference in the world for those who suffer with low back pain.