Having the ability to extend the thoracic spine is a game changer for many people, especially for those who tend to be sequestered for hours on end in front of a computer on a day-to-day basis.
For lack of a better term, a lot of cool shit happens with extension:
The shoulder blades can retract and upwardly rotate.
It’s much easier to get the arms overhead.
It’s easier to keep the chest up during squats and deadlifts.
It makes for a “better” bench press. I.e., shoulder blades can retract and depress providing a more stable base of support.
The thoracic spine (thorax for the nerds in the room) is the “anchor” of the shoulder blades. Ideally we like to see congruency between the ribcage/thorax/t-spine/whatchamacalit and the shoulder blades.
When someone is a bit more kyphotic (rounded) in that area it makes it almost impossible for this to happen because the shoulder blades will often be more abducted and anteriorly tilted.
This can setoff a domino effect of other shenanigans such as a narrowing of the acromion space (for example), which in turn leads to rotator cuff issues, which then leads to not being able to bench press without pain, which, as we all know, means the Apocalypse is upon us.
Let’s avoid the Apocalypse.
To that end I’d like to take this time to share some of my “go to” T-Spine Extension drills I use with my own clients and athletes on a weekly basis.
1. T-Spine Extension Off a Foam Roller (Performed In a Way That Doesn’t Make Me Want to Swallow Live Bees)
Likely the most recognizable drill many gravitate towards – and for good reason (it’s a good one) – is T-Spine Extension off a foam roller.
However, many tend to go waaaaaaay too far with their total range of motion on this to where it becomes more of a lumbar spine movement.
Here’s how to do it correctly:
2. Prone T-Spine Extension
I reserve “fancy” for choosing a nice restaurant for a date night with my wife.2
I don’t feel the need to get fancy with my T-spine extension drills.
The Prone T-Spine Extension drill is a fantastic way to build mid-back endurance.
3. Child’s Pose Back Extension Off Med Ball
What’s great about this variation is that when we adopt the “child’s pose” (knees tucked underneath) we OMIT the lumbar spine.
So now the only area we can get movement is the t-spine.
4. Pigeon Stance w/ Reach Through & Extension
Taking the previous concept and upping the ante a little bit is this exercise I “stole” from Dean Somerset.
If we want to talk about a drill that provides a TON of benefit for our training buck this is it.
Here we get a stellar hip mobility/glute stretch, while at the same time taking the lumbar spine out of the equation (because that’s NOT where we want movement from).
Too, with the reach through (and then extension) we’re getting a double whammy effect of mid-back mobility goodness.
NOTE: I like to add in an inhale (through the nose) on the reach through and then a FULL exhale (out the mouth) as the individual extends back up.
NOTE #2: My tricep looks fucking amazing in this video.
5. Wall T-Spine Extension w/ Lift Off
This drill is a doozy as well.
Pushing the hips back and “settling” into your accessible t-spine extension ROM is money enough for most people. But when you add in the end-range “lift off” (lifting the hands off the wall) at the end, it adds that little “eff you” component not many people will like.
Be careful not to crank through your lower back on this one!
This one is more challenging than it looks, so way on the side of conservative when choosing the loads you use.
I’m using a 10 kg kettlebell in this video and am pretty sure I blacked out after shooting this video.
Want More Shoulder Magic?
Join me IN-PERSON for two upcoming Fall workshops I am putting on. I cover shoulder/hip assessment, programming strategies, the concept of the TRAINABLE MENU, favorite Decepticons, and much, much more.
Being human means being enamored by a litany of things in the health/wellness/physical preparation realm. Some people are easily swooned by fancy watches and elaborate looking exercises
Others by cryochambers and Paleo recipes that taste like sawdust.
I am not here to play judgement police. For the most part, everything has a time and place3 and everyone responds differently to different things.
What works for me may not work for you (and vice versa). It’s all good.
Back in 2009-2010, while at Cressey Sports Performance, I was introduced to PRI (Postural Restoration Institute). As a collective, we adopted some of their principles & protocols (specifically positional breathing) and applied them to our athletes’ and clients’ programming, I’d say with a high degree of success.
In the years since, PRI has grown in popularity and is still something I “subscribe” to. However, the key term I want to highlight here is “some.”
I’ve adopted some of their principles.
The thing about PRI (for better or worse) is that it has an uncanny ability to suck people in and plop them into a never-ending rabbit hole of mystery and multi-verses.
Today’s guest post is via Boston-based physical therapist, Mike DeMille, and offers a needed perspective on this phenomenon.
(PS: I’d encourage anyone interested with PRI to check out Mike’s course/mentorship below).
In a world of biomechanics, neurology, complex chronic pain, and a desire to create resilience, it can be difficult to decide as a Physical Therapist or movement specialist what continuing education courses to take and why.
Personally, I have been a PRC (Postural Restoration Certified) Physical Therapist for five years, and anyone familiar with the Postural Restoration Institute (PRI) knows how easy it can be to go down the “rabbit hole”
Note From TG: I wrote a bit about this “rabbit hole” a number of years ago when PRI was first gaining steam in the S&C side of the spectrum. You can check it out HERE.4
After taking different courses, it can be very difficult to sift through the information and add principles to your practice (or programming), while leaving behind minutiae that ultimately won’t contribute to the further results of your clients.
What are those techniques, exercises, prehab/rehab protocol, cues, sick hip-hop rhymes that probably do not need to come along for the ride as you build out your systems as a coach?
That is exactly why we are here today.
After working in a cash-based Physical Therapy and Personal Training setting over the last four years and starting my own clinic (just outside Boston,. MA) I’ve developed rules (or tenets) of information to hold on to and which ones to leave behind.
Let’s dive in.
Think Practitioner/Coach, Speak Client
Your clients do not care what things are called, and neither should you.
Exhale, eccentrically orient, compress, early-mid-late stance, inhaling from an exhaled skeleton expansion, these terms can get complicated, if not bordering on someone speaking Elvish.
A general rule of thumb would be if you cannot explain a concept in very simple terms to your client, then you likely shouldn’t spend a ton of time thinking about it yourself.
I like to think of this as writing a letter with a big bold sharpie instead of a small fine pencil that is difficult to see and read.
For example, if you have a client who you feel like is in a position of lumbar extension and they need to learn how to exhale to help get them out of pain, then you can leave the messaging at just that.
You will create the buy-in from spinning a simple story and allowing your client to feel the difference when undergoing your program. You do not need to explain all of the varying “compensatory strategies” to them in an effort to create belief in your program.
This will more likely than not lead to confusion, in addition to increasing the urge they’ll want to punch you in the face.
Nothing Is New; It Just Has a Fancier Name
Remember that these principles existed long before the most recent course that you took. One of the biggest problems that I see mentees and fresh PTs and movement professionals face is shiny object syndrome.
Understandably, when you go to a course and watch someone’s shoulder flexion increase from 140 degrees to 8000 after a fancy breathing exercise, you want to give everyone that fancy breathing exercise.
Remember, there is a difference between a new technique that creates transient changes, and principles that create long lasting repeatable results.
Examples of a few principles that could make sense in a movement practice geared towards clients with pain:
Sound communication (avoiding nocebo).
Axial skeleton position that creates pressure underneath load bearing joints.
Progressive overload.
Does it feel less exciting to not be blowing all of your clients minds?
Sure it does.
But will these principles give you a sustainable business where you can more accurately sell results to potential clients?
Definitely.
Closing Thoughts
There is nothing wrong with taking new courses, finding helpful information, and creating buy-in with prospective clients, as well as appreciating the nuances of Physical Therapy and Strength and Conditioning.
But let’s not forget: the name of the game is being able to tie your name to something that can produce consistent results, and that is why we decided to take on this profession in the first place.
PRI Pique Your Interest?
Does this message resonate with you? Are you a Physical Therapist or movement professional looking to sift through the information and take the relevant principles into your practice?
Tyler Tanaka and I have created a community where we take individuals that are looking to finally apply the information that they have learned and effectively communicate with their ideal clients to build the business that they have always wanted.
This is your chance to learn the system of two PRC PTs and ask any and every question that you have ever had. In the 10 week Solidify Program you will undergo a detailed curriculum as well as take part in one on one Refinement calls to get your questions answered about those difficult patients that are the ”non-responders” as well as big picture questions about your practice and business.
Get your mind out of the gutter, I’m talking about muscles here…;o)
The Difference Between Good & Bad Stiffness
Having “tight” or “stiff” muscles is often viewed as a bad thing. Not losing a match of Squid Game bad, but bad nonetheless.
When someone presents with a (true) muscular length limitation there are increased risks of injury involved – strains, tears, explosive diarrhea5 – not to mention an increased likelihood of faulty movement patterns up and down the kinetic chain.
But injury isn’t always omnipresent.
Take any NBA basketball player through the FMS (Functional Movement Screen) – specifically the Active Straight Leg screen – and you’re bound to open up a can of epic fail.
NOTE:I personally don’t use the FMS currently when assessing/screening new clients. I took both modules several years ago and gained a lot of insight and knowledge. But in the years since I have gradually weened away from the FMS for myriad reasons. I know a lot of fitness professionals who still utilize it though and feel it’s a relevant talking point in the context of this post.
Many would be lucky to score a “2” (which is an average score), and many would showcase a right/left asymmetry, which, as we all know, means a baby seal dies.6
As a result, we’re quick to go into corrective exercise overdrive and implement every strategy under the sun that’ll increase hamstring length.
Ironically, it’s “tight hamstrings” that allow many NBA players the ability to do what they do so well. Namely, jump through the roof.
In this case stiffness is a good thing. We don’t have to fix it.
Of Note:the ASLR screen isn’t necessarily a hamstring length screen to begin with. Sure, offhand, it can be a way to ascertain hamstring length…but what we’re really looking at is the ability to both flex and extend the hip.
Stiff hamstrings can affect the ability to do so. However, more importantly, the ASLR is about teaching people to get into better positions – improving stiffness in other areas – to “trick” the CNS into turning off the emergency breaks.
Get people into more optimal positions (nudge them into better alignment), and what presented as “tight” or stiff is no longer the case.
Core Engaged Active Straight Leg Raise
Here we engage the anterior core – increase stiffness – to promote more posterior pelvic tilt (decrease “bad” stiffness in lumbar spine) in order to improve ROM, in addition to getting movement from the right areas (in this case the hips).
Likewise we can throw the hip flexors underneath the bus. I think we all know someone who’s been stretching their “tight” hip flexors since 1997.
Newsflash: If you’re someone who’s been mindlessly stretching your hip flexors for that long, with no improvement, what the hell?
I’d garner a guess the reason they feel tight/stiff is due to protective tension (and not actual tightness).
The stretch you’re doing – what I like to call the BS Hip Flexor Stretch – is doing nothing more than increasing “bad” stiffness in the:
Lumbar spine.
Anterior hip capsule.
My eyes.
It exacerbates and feeds what’s causing the issues in the first place.
Instead, perform a REAL Hip Flexor Stretch by increasing (good) stiffness in the appropriate areas – the anterior core and glutes – and actually get at the crux of the issue.
Another prime example would be the lats.
Stiff lats can be a bad and a good thing.
When Shit Hits the Fan (I.e., Bad)
In mine and Dean Somerset’s Complete Shoulder & Hip Blueprint, we spend a large portion of time speaking about the lats and how, in the overhead athlete population (as well as in the general population), they’re often stiff/short and overactive.
As a result: Overactive/stiff lats will drive more shoulder depression, downward rotation, adduction, as well as lumbar extension in general.
Anyone familiar with PRI (Postural Restoration Institute) and their thought process and methodologies will recognize this “Scissor Posture,” where the pelvis is pointing in one direction (tilted forward in Anterior Pelvic Tilt) and the diaphragm pointing in another direction (due to an excessive rib flair and lumbar extension).
This is not only an unstable position to be in, but also keeps the nervous system “on” at all times, driving more sympathetic activity.
What’s more, with regards to shoulder health, overactive lats will make it much less likely someone will be able to elevate their arms overhead, as well as “accessing” their lower traps (which share a similar fiber orientation as the lats @ 135 degrees), which, in concert with the upper trap and serratus, aid scapular upward rotation, posterior tilt, and protraction.
Taking the time to coach someone to turn off (or down-regulate) their lats in order to flex, externally rotate, and abduct their shoulder works wonders.
Bench T-Spine Mobilization
Wall Lat Stretch w/ T-Spine Extension & Lift Off
When Lats Can Increase Your Overall Level of Badassery (I.e., Good Stiffness)
And now it’s time to turn those fuckers on!
Your lats are a MAJOR player when it comes to performance in the weight room and lifting heavy things.
It also behooves you to turn them on in order to improve your technique in the “big 3.”
With the deadlift in particular there are some significant advantages:
Another trick I like to use to help people learn to use their lats during a deadlift is to attach a band to the bar and a stationary object.
Trainees will learn very quickly what it means to “pull the bar towards you” and to keep the lats engaged throughout the duration of a set.
You can also peruse a few more options in this IG post from a few weeks ago:
…it’s not always end of days or something that requires going into DEFCON 1 corrective exercise purgatory mode. Whether or not stiffness/tightness is bad or good depends on the context.
Single leg training isn’t sexy to talk, much less write about. In terms of excitement factor I’d rank it somewhere between a watching a NASCAR race and picking lint out of your belly button.
I can understand the cacophony of subsequent eye rolls and yawns that are being directed my way.
“An article on single leg training?! Come on, Tony. What’s next keto recipes?”
5 Ways I Include Single Leg Training In My Programs
Single leg training is important shit.
Now, more often than not whenever there’s an article written on single leg training it’s under the guise or in congruence with taking a massive dump on bilateral training (think: squats and/or deadlifts).
The implication being one should avoid bilateral or two-legged training in lieu of performing only unilateral or one-legged training.
I think it’s a stupid argument to have on par with which is better: Low-bar vs. high-bar squats? Or mint chocolate chip vs. mint Oreo ice-cream?
With deference, almost always, the appropriate answer to the single leg vs. bilateral debate (and, really, any question in the history of ever) is “it depends.”
Some people are more concerned with being brutally strong with the “Big 3” and are only worried about optimal force production. If that’s the case bilateral movements should make up the bulk of training.
Conversely, some people, especially athletes, need to marinate in a diverse pool of movement. In that case single leg training is going to take precedence and play more of an integral part in their training and programming.
Are there people out there who debate ice-cream? Don’t be cray-cray.
Suffice it to say, here’s my take on the debate: BOTH are important, BOTH play a significant role in a well-balanced program, and BOTH should be used simultaneously.
If we’re being honest, though, we generally don’t have to pull any arms behind backs in order to convince people to perform bilateral movements like squats and deadlifts.
It’s pretty much bro-code.
Single leg work on the other hand?
Well, that can be a bit of a harder sell.
It’s unfortunate because even if someone’s goal is to be a brick shit house (or a house of shit bricks, I’m not here to judge) single leg training has many benefits, mmmkay.
Including but not limited to:
Joint health and integrity (I have yet to find an individual with a history of knee, hip and/or back issues who doesn’t benefit from a healthy dose of single leg training).
Improved balance.
Improved foot/ankle/hip stability. Or, stability in general.7
A fantastic way to train rotary stability (<— a fancy schmancy way of saying something will work your core).
Greater specificity to sport (and real life).
Improved strength & hypertrophy (depending on how it’s implemented).
Helps address weaknesses and imbalances from limb to limb.
Below are (some) ways I like to include single leg training in my programs.
1) Treat Single Leg Training Like Eating Broccoli
It’s just, you know, something that has to be done.
It’s hard for me to peruse the list I made above of all the benefits and not include some semblance of single leg training in a program (regardless of someone’s goal).
There aren’t many scenarios I can think of off-hand where it won’t help.
Be a better athlete? Check
Be a better lifter? Check
Beat Jason Bourne in a knife fight? Check.
All the bases are covered.
That said, one pet-peeve of mine and something I notice all….the…..time as a coach is that people tend to go way too heavy.
I’ll watch some guys grab the 80+ lb dumbbells and perform walking lunges and think to myself “why?”
But this is after both my corneas jump out of their eye sockets and then proceed to jump into a bucket of battery acid.
Their knees are caving in every which way and it’s evident most are unable to control the load. This kinda defeats the purpose of doing it in the first place.
Stop training your ego and lower the load.
I’d rather people use a load they can control and perform it for high(er) reps than to grab the heaviest weight possible and make perhaps do more harm than good.
ALSO…..
It’s my own preference as a coach, but I much prefer people to adopt more of a forward lean when performing lunge variations.
When you assume a more upright posture during lunges it makes it easier to crank through the lower back which can also result in excessive rib flair; I.e., a more unstable position.
The inner dialogue should be more “shoulders over knees” than “shoulders over hips.”
2) Potentiation (Or, Turning “Stuff” On)
I often have my clients perform a single leg movement before squatting or deadlifting.
https://www.youtube.com/watch?v=a1Y73sPHKxw
I find it’s a nice way to turn “stuff” on and to prime the body for the extracurricular shenanigans going down shortly thereafter.
Goblet variations are my go to here (less grip intensive): Goblet Reverse Lunge, Goblet Forward Lunge, Goblet Reverse TO Forward Lunge, Goblet Split Squat, Goblet Bulgarian Split Squat, Goblet Whateverthefuck.
The idea is to go LIGHT and to OWN the movement.
I like to use 2-3 sets of 6-8 reps per side.
Pants optional.
3) Adding Isometric Holds
If you really want to humble someone (and to make their glutes scream for blood mercy) try adding in some isometric holds.
I LOVE using these with my clients/athletes as it forces them to use sloooooow down, to stay more cognizant of body position, and it also aids in more time under tension.
4. Combo Movements
Another way I like to include single leg training into my programs is to combine two movements into one.
This is a fantastic way to make the movements a bit more challenging and also serves as an opportunity to stroke my evil strength coach beard (despite the fact I don’t have one).
You want sore, I’ll give you sore.
Goblet Step-Through
Rear Foot Elevated Kang Squat
5) Fake Single Leg Training
Least we forget single leg training can be too advanced of an option for some people. Whether it’s due to novelty or “just because” we can incorporate “fake” single leg options to help ramp people to the real thing.
I’m more concerned with setting people up for as much success as possible rather than making them feel frustrated.
In that light here are two excellent options I use all the time:
Wall Press RDL
Here, we can still groove a single leg hinge pattern, but in a supported fashion.
For those who have balance issues this is an excellent choice.
B-Stance Squat
With the offset (or B) stance, we place more load on the front leg. Again, this is a great option for those with stability/balance issues and who aren’t quite ready for actual 1-legged squats (you sadistic bastard).
Do you exhibit a hip/weight shift (swaying to the left or right) when you perform a squat? It’s one of the more annoying things that can happen in the weight-room.
It ranks somewhere in between people who don’t re-rack their weights and kipping pull-ups.
Admittedly, it’s rather common and almost always a benign occurrence; most people never even notice it unless they’re routinely filming their squat sessions.
And when that is the case, I can understand someone’s “itch” to want to solve the conundrum. I mean, things could go awry down the road and manifest into pesky hip or knees issues.
A Case Study: How to Address a Hip Shift During the Squat
I received the following email earlier this week:
“I was looking to see if I might be able to send you some videos for a squat assessment. I have been having issues leaning to my right for some time and cannot for the life of me figure out what is causing the issue. I’ve followed you for years and trust your judgement!”
I responded back with a “sure, I can take a quick look,” and in swift fashion I got this in return:
“Some initial feedback would be great.
Some things to note before watching:
Though subtle, I find my left hip lower than my right on both the descent and ascent of the squat (as you can probably see).
My right hip flexor/quad tends to be tighter than my left usually.
My left glute has always been tighter than my right
History of SI joint hypermobility (in the past) but has not caused me issues for over a year. I used to have issues with my sacrum shifting around and causing misaligned hips which was quite painful.
I do not have any pain barbell squatting or semi sumo deadlifting but I do feel the unevenness when I squat especially.”
https://www.youtube.com/watch?v=-OGaW1JmADw
For Starters
That’s a pretty good lookin squat if you ask me.
After reading her “heads up” commentary before watching the video I was half expecting a dumpster fire when I pressed play.
Au contraire – all things considered, that’s a very passable squat.
However, given her past injury history, her own words of feeling the “unevenness,” not to mention you can see a subtle weight shift to the right with each repetition, I had some thoughts.
It’s funny, I perused my blog archives to see whether or not I had written on this topic in the past, and as it happens I did!
Back in 2015 I wrote THIS post where I discussed the idea “feeding the dysfunction,” a concept taken straight from renowned physical therapists (and creators of the Functional Movement Screen), Gray Cook and Lee Burton.
The gist goes like this:
You see a weight shift, say, to the right. In this scenario you grab a band and wrap it around the individual’s waist and as he or she squats, you pull the band in the direction of the shift, essentially “feeding the dysfunction.” The idea is that reactive neuromuscular training (RNT) trains the nervous system to recognize a faulty movement and to encourage body to correct course.
In the broader consciousness of health/fitness it’s an okay approach. It 100% works. In the years since writing that blog post, however, I’ve gone out of my way to reduce my use of the word “dysfunction” with clients. I don’t like the connotation the word breeds; that the individual is in some way broken or needs fixing.
Some people hear or see the word dysfunction and they’re ordering an exorcism.
Myself?
I hear or see dysfunction and I think “well, outside of extenuating circumstances (past/current injury history, whether or not there’s pain present), it’s fairly normal.”
Everyone is a bit different and moves in different ways. What’s more, there are, what, seven billion people on this planet currently? Is the expectation that everyone, everywhere, in the history of ever, is going to squat (or move) the same exact way?
Okay, Tony, We Get It, Personal Growth, Blah Blah, Blah…WTF Did You Tell Lisa To Do?
This, I said this:
“I totally see what you’re saying when you say your left side is lower than your right. I don’t think we need to get too far into the weeds as to whether or not that “needs” to be corrected (or even if it’s bad).
While slight, the hip shift IS there, and I think there are one of two things you can try”
1) Lean Into the Asymmetry
(NOTE: I actually wrote my thoughts on asymmetry HERE a few years ago).
I asked her to externally rotate (open up) her right foot more and to take note whether or not that improved her weight shift?
If so, there’s her answer.
People are built differently and what this would suggest is that her right hip socket is likely more retroverted compared to her left and that that side requires a bit more ER.
For many, using a “symmetrical” stance is akin to attempting to fit a square peg into a round hole. We don’t live in textbooks, so we shouldn’t train like it either.
She tried it and (no surprise to me) saw an improvement:
https://www.youtube.com/watch?v=CcKlqEkC8EI
But Tony, Won’t Having Her Squat With An Asymmetrical Stance Lead to More Issues Later? What’s Next: Telling Her to Club a Baby Seal? No, Wait, To Go Keto?
Relax.
I truly don’t feel having someone perform a handful of sets with an asymmetrical stance is going to cause irreparable harm. I mean, I’d make the case that forcing symmetry is leading to more issues. Besides, if a certain stance feels better, feels more secure, stable, and powerful…why wouldn’t we want to lean into that?
Furthermore, the human body is a bit more resilient than that. If it can survive plagues, saber-toothed tigers, and Michael Bay Transformer movies, it can withstand a few sets of asymmetrical squats.
Further furthermore, this is why we use things such as single leg work to help fill in the gaps. There’s a reason why we write well-rounded training PROGRAMS. You know, to address stuff.
So anyway, moving her foot out a bit seemed to have solved the issue. This strategy will work for most people, but what happens when it doesn’t?
2) Listen to Katie St. Claire
This scenario reminded me of something my colleague, Katie St. Claire, discussed last year. She showed a video of one of her clients who also had a hip shift to the right on her squat.
Katie recommended the woman perform 15 hip bridges (off the wall) on her LEFT side only.
Now, why the LEFT side only in order to fix a RIGHT sided issue?
“To allow more posterior rotation and nutation on the left side so she can load the right side correctly.”
In non-Elvish, as you squat down into deeper hip flexion (most often in Stage 2: 60-120 degrees of hip flexion), the inability for the LEFT side to internally rotate and compress essentially “pushes” you to the right.
I don’t know, maybe that still sounds confusing.
Try this: Whatever side you shift to, perform a boat-load of bridges on the OPPOSITE side. Chances are you will see an improvement.
Cool?
Cool.
Give both options a try and see if one of them solves the issue.
I’ve always prided myself in my ability to recognize (and then attempt to address) my knowledge gaps.10
Understanding functional anatomy? ✅
Peeling back the onion on the importance of breathing mechanics? ✅
Having a better understanding of how to appropriately program plyometrics? ✅
Long division? ❌
One of the best things I did for my career, however, was to better educate myself on the topic of training clients’ through pregnancy in addition to having a better understanding of the intricacies working with postpartum women.
Anyone who works with women – which is pretty much every coach, ever – should consider investing in this area. I can only speak for myself, but studying this topic in more depth has given me much more confidence as a coach.
I’m also speaking for myself when I say one of THE best courses I have ever taken – not just on the topic, but ever – is Dr. Sarah Duvall’s Pregnancy & Postpartum Corrective Exercise Specialist course.
34 hours of content (legit, everything is covered: The only thing not covered is showing a live birth).
CEUs available (the total # will depend on your certifying body).
Payment plans are available too.
I cannot express enough how valuable this course has been in helping me not only become a better coach, but also gaining the confidence/trust of my female clients. I have little reservations in saying that investing in this course will pay for itself tenfold.
Below is a repost of an article I wrote last year sharing some of the things I’ve learned taking the course. But for those who prefer to skip the foreplay, you can go HERE to purchase. REMEMBER: The discounted price only lasts through Wednesday (2/24).
Outside of that, you should totally read my article (pretty sure it’s Pulitzer worthy).
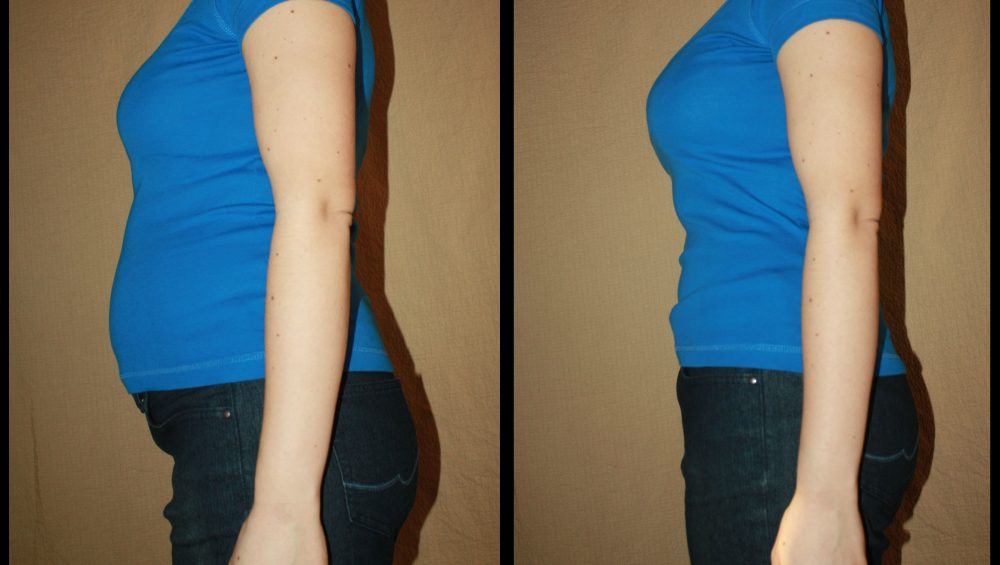
4 Things to Consider When Working With Postpartum Women
1. Once a Woman is Postpartum, She’s ALWAYS Postpartum
This is a powerful quote and something Sarah stresses over and over again in her course. Whether you’re working with a woman who is very recently postpartum or she gave birth three years ago, you still need to do your due diligence as a coach.
Just because some time has passed doesn’t mean she’s out of the weeds yet. Some women exhibit significant Diastasis Recti years after giving birth and shrug it off as “meh, that’s just the way things are.”
Likewise, some women view incidents such as incontinence (urine leaks) as equally “normal” and shrug worthy years after the fact.
NEWSFLASH: they’re not.
In light of that, it’s important to ask questions and to peel back the onion on a woman’s (reproductive) health history to glean as much information as possible.
Now, I get it: I’m a dude.
There’s a high degree of professionalism at play here.
“So, where you from?”
“Born and raised in Boston.”
“Awesome, do you have any major injuries I need to be aware of?”
“Nope, none I can think of.”
“How many kids do you have? Did you have a natural birth or c-section? Oh, and do you pee when you squat?”
To help stave off any awkwardness, I’ll send all prospective clients a questionnaire to fill out a head of time with pertinent questions related to this part of their health history.
If they’ve never given birth then they can skip and move on to the “Favorite Movie of All-Time” section (which is TOTALLY a thing by the way. I find it’s a great conversation stimulator and helps break the ice). And if they do have kids I ask them to fill out that section which has a handful of follow-up questions.
They can then go into as much detail as they feel comfortable with with 1019% less awkwardness.
That’s the order of things you’ll almost always want to prioritize when working with postpartum women. I’ve had a crush on the importance of positional breathing drills ever since my days at Cressey Sports Performance.
We found there was a lot of efficacy towards their use with getting athletes into a better position prior to training; specifically nudging toward a canister position (Zone of Apposition, I.e., the act of bringing things together or in proximity) as opposed to a scissor position.
Canister Position = diaphragm and pelvic floor stacked on top of each other.
Scissor Position = the opposite of that.
The latter tends to be a much more UN-stable position and can (not always) result in a fusillade of things we’d rather not see happen:
Poor breathing mechanics.
Lower back pain.
Shoulder pain.
Many of the things I’ve already noted above: DA, pelvic floor issues, etc.
Global warming
Another Transformer movie.
Honing in on breath can help “glue” or connect things more efficiently. Making sure someone is getting 3D expansion of their rib cage (and not just breathing UP into their chest) can be a game changer and helps to set the stage for everything else that follows.
If you don’t own breath, you’re not going to own “position” during exercise.
Something as simple as the Deadbug exercise – done correctly, with emphasis on the breath – is a great example.
It’s important to note that everyone is different and every birth is different. I can’t stress enough the importance of encouraging a woman to wait until she’s ready before implementing any mode of exercise. However, it’s important to note that it only takes 14 days of bedrest to notice atrophy of the Multifidi and surrounding spine musculature.
Encouraging small walks in conjunction with very basic breathing drills can help offset this.
Reiterate – from the rooftops – that a woman’s core is GOING TO BE WEAK FOR A LONG-TIME and that it is okay, normal, and 100% human for this to happen.
It still behooves them to set in motion – when they’re ready – these mini interventions that will pay HUGE dividends down the road.
3. It Takes Time
Women who train during their pregnancy are often the most vulnerable. They want to revert back to their “normal” training schedule often times before they’re close to being ready.
The pelvic floor (and other places of trauma) need time to catch up.
A good rule to keep handy:
“9 months to grow, 9 months to recover.”
This is not to imply that a woman can’t start lifting weights or exercising more vigorously prior to nine months, however it’s just to toss in a bit of expectation management.
The kipping pull-ups and heavy squats can wait.
FIRST FOUR MONTHS = rebuilding solid base (get the pelvic floor and core working with a ton of breathing drills).
But even this approach can be tempered to that of the client and her capabilities.
As an example I have a current client who gave birth less than a month ago who has just started to come back to the gym to train. She had been working with me for two years prior and knows her way around the weight room.
Here’s an example of her first week of training back:
D1. Box Jumps – AMAP x 2x30seconds
D2. Just kidding. The fuck outta here.
Again, everyone is different.
The umbrella theme to remember, though, is to TAKE THINGS SLOW!
4. What To Avoid in the Early Stages
On that front, here are some thing you’ll likely want to skip altogether in the early stages of working with postpartum women:
Plyos – burpees, jumping jacks, stairs, stop it.
Running – just an accentuated plyometric.
Front Abdominal Exercises – planks, sit-ups, push-ups, leg lifts (or anything that makes the abs bulge in front or uses the core to support a lot of the body weight).
Ninja Fights – Probably best to avoid ninjas at all costs, actually.
And That’s That
There’s obviously a lot more to consider, but that’s a pretty good start. For much, MUCH more on this topic check out the Certified Pregnancy & Postpartum Corrective Exercise Specialist 2.0 course HERE.
Your face is going to melt so hard you’ll learn so much.
Hi, my name is Tony and I ruptured my Achilles tendon earlier this year.
It was the first significant injury of my life and one that, as it happens, happens often (and without warning). Since my injury six months ago I’ve met numerous people who have gone through the same dumpster fire of an experience.11.And as a result I’ve documented my rehab and post-surgery training via my IG account using the hashtags #findyourtrainablemenu and #achillesgate2020.
However, I figured something more in depth and robust with regards to explaining the mechanism of Achilles rupture (as well discussing prevention) could be of benefit to the masses. To that end, my fellow coaches and colleagues – Dr. Bo Bobenko and Shane McLean – offered to write something for the site to cover exactly that.
For what it’s worth: I peppered in a few comments myself along the way.
Measures to Strengthen & Prevent Achilles Injuries
When admiring yourself, flexing away, do you ever give thought to the unsung hero of muscle? You know, the things that attach the muscles to your bones: the tendons. You probably don’t give much thought, until it’s too late.
Unless you’ve had your head in the sand, you know our resident funny man and light saber fighter extraordinaire, Tony Gentilcore tore his Achilles tendon while hanging out with the in-laws in Florida six months ago
NOTE FROM TG: It’s important to remember that correlation doesn’t equal causation here. My in-laws didn’t cause my Achilles rupture…;o)12
Tony, a big strong guy with no history of serious injury performs a drill he has done before and boom, suddenly it’s not his day, week, month or even his year….
NOTE FROM TG: For those interested, HERE is a great depiction of the exercise (and mechanism) that served as the impetus to my injury.
The “Jump Back” Start
This video almost exactly showcases what happened. The only difference is that I didn’t preload my sprint with a three-hop thingamajig (just one), and in my case, once my back leg planted, I fell immediately to the ground.
Plus I may or not have been wearing a cape.
A Little Background On The Achilles Tendon
The tendon is named after the ancient Greek mythological figure Achilles (and not Brad Pitt) as it was the only part of his body that was still vulnerable after his mother had dipped him into the River Styx. Plus, we all know where he got shot with an arrow, at least in the movie.
The Achilles tendon is the thickest and strongest tendon in the human body. It’s the tendinous extension of the three-headed calf muscle soleus and the two-headed gastrocnemius and it inserts on the calcaneus (heel).
The contraction of the calf muscles transfers a force through the Achilles tendon, which enables plantar flexion of the foot and allows for actions such as walking, running, jumping, bounding, sprinting, and skipping.
During these movements, the Achilles tendon is subject to the highest loads in the body, with tensile loads up to 10 times the body’s weight.
The reasons for this are twofold: First, the Achilles consists of type II fast-twitch fibers, and this elasticity allows for rapid forward and backwards movement. Secondly, the tendon type I fibers of collagen and elastin which are lined up parallel from calf to heel, are responsible for the Achilles tendon strength. (1)
The Achilles due to its strength and its ability to handle high loads makes it a resilient tendon, which is good and bad. Good because it can handle lots of load and bad because it’s not always going to send pain signals to the brain every time something goes wrong.
This is one reason why Achilles tears can happen without warning.
Types Of Achilles Injuries
When your achilles hurts or you feel pain you’ll often be told ‘You got tendonitis bro’ But there are few different types of Achilles injuries besides tendonitis.
1. Achilles Tendon Tears
This is the mack daddy of all tendon injuries and like with Tony, it often happens without warning. If you hear a pop and a pain that radiates up your lower leg, there’s no second guessing what you’ve done.
NOTE FROM TG: The best way I can explain the sensation is that it feels like someone taking a sledgehammer right to your ankle. It doesn’t tickle.
2. Achilles Tendinopathy
Tendinopathy is a degeneration of the collagen protein fibers that form the Achilles. Its symptoms include increasing pain at the heel, stiffness, swelling at the back of your ankle, and a grating noise or creaking feeling when moving your ankle.
3. Achilles Tendonitis
Tendonitis is acute inflammation of the tendon and its symptoms include pain and stiffness in the morning, pain that worsens with activity, extreme pain the day after exercise.
There are two types of Achilles tendonitis: insertional and noninsertional.
Insertional Achilles tendonitis affects the lower portion of your tendon where it attaches to your heel bone often caused by bone spurs.
Noninsertional Achilles tendonitis involves fibers in the middle portion of the tendon.
4. Achilles Tendinosis
Tendinosis is the non-inflammatory degeneration of the collagen fibers of the tendon. This includes changes to the structure or composition of the tendon that results from repetitive strains without proper healing.
Achilles and calf tightness are common causes of Achilles tendinosis. Plus insertional Achilles tendinosis is often associated with heel spurs as it rubs against the achilles causing small tears.
Activities That Cause Achilles Tears
Achilles tendon tears happen to people who do things where they quickly speed up, slow down, or pivot, such as:
Running
Gymnastics
Dance
Football
Baseball
Softball
Basketball
Tennis
Fighting Zombies, Salsa Dancing, Talking About Feelings (<— things added by Tony)
Achilles tears tend to happen when you start moving suddenly as you push off and lift rather than land. Sometimes these abrupt actions can be too much for the tendon to handle.
Here is the statistical lowdown on how tears happen.
90% of injuries occur with an acceleration/deceleration movements mentioned above
Only 15-20% of men reported any sort of heel pain/tendinosis before the injury
50% of men who have an Achilles Rupture had tissue degeneration before the injury
Typically occurs 30 minutes after moving around
Research has shown Achilles tears include clear degenerative changes before the rupture but many of the Achilles tendon ruptures occur suddenly without any preceding signs or symptoms. (2)
For instance, Tony’s tear was caused by aggressive eccentric load (jump back start) combined with poor load management and then “jumping” right back into sprinting.
NOTE FROM TG: Exactly. Part of the problem was sheer bad luck. But too, up until that point – eight or so weeks into pandemic quarantine – I hadn’t been doing much (if any) plyometric activity.
In his mind it was all systems go. The main point here is there’s not one definitive “cause.” of Achillies tears. It’s equal parts shit-happens and bad luck.
Big Picture With Tendon Pain Modulation
1. CNS Response
The CNS is incredible at responding to and adapting to pain modulation. This is a good thing to keep going and for our survival but makes understanding our tendon health much trickier because damage can exist without pain.
2. Load Management and Exposure
This is probably the single most important component to tendon health that we should seek to understand and pay attention to. It can be intimidating to truly track your loads/exposure, but the better we get at it, the more we increase our chance of avoiding injury.
All of the research continues to bear out controlling the load on tendons is the best way to make any kind of change. The analogy I often use when explaining this to patients is the comparison to a wall that continues to take damage or have a crack and we need to keep adding spackle to it every 48 hours to reinforce it and strengthen the overall structure.
How To Prevent Achilles Tears
The experts and research are a bit mixed on this therefore the safest approach in my mind is to increase the variety of loads you place on the tendons.
Unless training for a specific sport or activity, then we should focus on preserving the natural capacity of what the tendon is meant to do, which is to absorb and transfer forces effectively in the simplest of terms.
Pogo Jumps
Heel Taps
A Daily Routine to Incorporate Into Your Movement Prep
You need tendon loading with multiple angles and a plan for tempo for the long term. My go to is often for heavy slow resistance, four seconds eccentric, three seconds concentric, carefully plotted over 12 weeks. There is strong research to support this concept.
A quote I really like about this:
“We start dying when we stop jumping.”
Assessment can be vital, but there is no Gold standard. Personally, I use my hands to assess pain tolerance to pressure at the tendon as one way to track progress of tendon health, but this is not well supported by research and requires me to have physical access to you which can be limiting indeed.
If you haven’t loaded the tendon recently, some easy options are
Calf raises with full range of motion, faster up slower down, aiming for 20 reps per leg as a baseline for tendon health. This allows us to look for asymmetries as well as an overall deficit based on training age.
In terms of a plan to increase your activity tolerance:
Firstly, I like to think of the principle of 10% per session as a safe progression. Meaning, in terms of a weekly volume a nice progression is to add 10% to the previous week.
Secondly, the quote that drives me here is:
“We tend to overestimate what we can accomplish in a month and underestimate what we can accomplish in a year.”
Therefore, a long term strategy for tendon health should be implemented.
Exercise Is Important But So Is Diet
It goes without saying reducing stress, sleeping soundly, and eating nutritious foods not only helps you…
…but your tendons specifically.
But I said it anyway.
However, there are a few supplements on top of eating and sleeping well, reducing stress and moving better which help heal and keep tendons resilient. Notice the word supplement. These should NOT be your priority to help your tendons stay healthy or heal after an injury.
Primary should always be eating real high quality foods.
The first and most obvious supplement is Vitamin C.
Vitamin C is absolutely essential for synthesis of collagen which makes the tendons type 1 slow twitch fibers strong. Pre clinical studies have shown vitamin C has the potential to accelerate bone healing after a fracture, increase type I collagen synthesis, and reduce oxidative stress after a tendon injury. (3)
Supplementing with Vitamin A helps the process of forming new tissue (collagen) and your immune system. A stronger immune system can prevent microorganisms from further damaging your tendons.
Vitamin E has anti-inflammatory properties which helps reduce tendon inflammation, and helps the healing of damaged tendons which can lead to a reduction of tendon pain. (4)
The science and research is limited on diet and tendon health and there are probably other things out there that can help. It is an ever expanding field so stay tuned.
NOTE FROM TG: At the moment, I like the Collagen Peptides from Momentous because they use Vitamin C, and FORTIGEL® , which is a formula designed and tested to promote collagen synthesis in tendons and ligaments.
(👆👆👆 Discount:GENTILCORE25 gets you 25% off your first order when you sign up for a subscription 👆👆👆)
Most collagen out there is basically like buying a pack of J-E-L-L-O, focusing on hair, skin and nails, but this stuff is solid and provides a bit more heft.
Here’s the daily “Wolverine Cocktail” I’ve taken every day since my surgery on June 1, 2020:
Tendon tears often happen without warning and it doesn’t discriminate on whether you’re fit or not. One moment you’re about to move quick and the next you’re on the ground.
The best things you can do before engaging in risky tendon activities:
Warm up properly
Load the tendon appropriately
Reduce stress, eat and sleep better.
But as you’ve seen by Tony’s experience, there are no guarantees. Please do your best so you don’t hear the pop from hell.
Authors’ Bios
Shane “Balance Guy” McLean, is an A.C.E Certified Personal Trainer working deep in the heart of Louisiana with the gators.
Dr. Bo Babenko is the owner of FitCare Physio focusing on virtual health coaching and helping people attack the 5 pillars of health: movement, nutrition, recovery, mindset, connection.
References
Michael Wong; Achraf H. Jardaly; John Kiel.Anatomy, Bony Pelvis and Lower Limb, Achilles Tendon.
Nicholas N DePhillipo et al. Efficacy of Vitamin C Supplementation on Collagen Synthesis and Oxidative Stress After Musculoskeletal Injuries: A Systematic Review. Orthop J Sports Med 2018 Oct 25;6(10)
Christopher Tack,Faye ShorthouseLindsy Kass. The Physiological Mechanisms of Effect of Vitamins and Amino Acids on Tendon and Muscle Healing: A Systematic Review. Int J Sport Nutr Exerc Metab 2018 May 1;28(3):294-311.
Exercises You Should Be Doing: Wall Press Rotation
When it comes to dealing with hip shenanigans13 I think we’ve done a pretty solid job as an industry at prioritizing OPEN chain exercises.
For those not in the know, open-chain exercises are where…
“…the segment furthest away from the body – known as the distal aspect, usually the hand or foot – is free and not fixed to an object.”
This would make a lot sense given the hip joint – which is a ball and socket joint – is an area designed to be mobile. I don’t need to belabor the point here as there’s an abyss of exercises & drills to choose from.
But you can also peruse Instagram and it won’t take long before you find someone contorting themselves like a pretzel in the name of likes and five seconds of fame.
Which leads to a not-so-obvious digression.
Lately, after having listened to and corresponded with a few of my colleagues, I’m beginning to realize that open-chain exercises are just HALF the answer.
Closed-chain drills need some love too.
Wall Press Rotation
Who Did I Steal It From? – A rockstar (metaphorically speaking): Katie St. Claire. You should give her a follow. She’s legit.
What Does It Do? –
1️⃣ This drill works on pelvic range of motion, but as the preface implies…in a closed chain fashion. The advantage here is that it emphasizes acetabulum motion over a fixed femur.
It feels amazing and serves as a nice drill to implement before some squats or deadlifts.
2️⃣ Too, and as Katie has pointed out, this drill also hammers home foot mechanics. As I flex into hip internal rotation I drive more foot pronation. Conversely, as I extend into hip external rotation I drive more foot supination.
A splendid drill that marries together hip-foot mechanics.
Key Coaching Cues – I’m holding onto an EZ-curl bar, but anything similar – PVC pipe, light barbell, Nimbus 2000 – will do. Be sure to press the rear foot into the wall. You’ll then flex/rotate into hip IR on the standing leg while also accentuating a full exhale.
Exhale into the stretch.
Reverse your action, rotating back/extending as you inhale.
You can’t go more than a few clicks on the internet before you inevitably come across some coach or trainer discussing the merits of positional breathing and how it can help improve performance in the weight room (and on the field).
(👆👆👆 I guess this depends on what part of the internet you peruse…BOM, CHICKA, BOM BOM 😉 😉 😉 )
Nevertheless, if you’re someone who geeks out over the human body and movement in general “positional breathing” is a term you’ve definitely come across.
And you likely still aren’t understanding it’s relevance.
I have a treat for you today. Dr. Michelle Boland (a Boston based strength & conditioning coach and one of the smartest people I’ve ever met) was kind enough to offer to write on the topic for this website.
Positional Breathing: The Implementation of Training Principles
Note From TG: For a bit of an “amuse bouche” on the topic of positional breathing I’d encourage you to check out two posts I wrote on the topic HERE and HERE.
Identify
Our role as fitness professionals is to determine what is important for our clients. In order to do so, we need to identify what is important, formulate principles, and then follow through with implementation.
A way to identify and formulate what is important to us as trainers, is to create principles. Principles are simply what you believe in and what you teach your clients. Principles serve as a hierarchy of reasoning for your training methods, which include your choice of exercises, organization of training sessions, program design decisions, and communication strategies.
In this article, I am going to review my first two training principles:
Training Principle 1: All movement is shape change (influence from Bill Hartman)
Training Principle 2: Proximal position influences distal movement abilities
Formulate
Movement is about shape change.
We change shapes by expanding and compressing areas of the body.
Movement will occur in areas of the body that we are able to expand and movement will be limited in areas of the body that, for some reason, we have compressed. The ability of an athlete to transition from expanded positions to compressed positions informs their ability to change shape and express movement.
Movement occurs in a multitude of directions depending on both position and respiration. Certain positions will bias certain parts of the body to be able to expand more freely, allowing increased movement availability. Respiration can further support the ability to expand and compress areas of the body, as an inhalation emphasizes expansion and an exhalation emphasizes compression.
(👇👇👇 Just a small, teeny-tiny taste of importance of positional breathing 👇👇👇)
Position selection is my foundation of exercise selection.
Positions such as supine, prone, side lying, tall kneeling, half kneeling, staggered stance, lateral stance, and standing can magnify which areas of the body that will be expanded or compressed. Additional components of positions can include reaching one arm forward, reaching arms overhead, elevating a heel, or elevating a toe. Furthermore, pairing phases of respiration within these positions will further support where movement will be limited or enhanced.
The position of the proximal bony structures of the body, such as the rib cage and pelvis, can greatly enable or restrict movement. Positional stacking of the thorax and pelvis provides an anchor for movement. Respiration then provides the ability to create expansion in the thorax and pelvis, thus providing expansion areas of the body, within joint spaces, allowing our limbs to express pain-free movement.
Lifting heavy weights can often compress areas of our body and reduce our ability to expand and rotate through our trunk and hips, limiting movement, and negatively affecting our ability to perform. Remember, expansion begets movement freedom, so adding positional breathing work or pairing movement with respiration can create opportunities for expansion.
Implement
Where is a good place to start with positional breathing work?
Start by thinking about what you already do.
Then, apply your new lens of where you want movement to occur.
Finally, label the positions of the exercises and pair respiration within those movements. Pair an inhalation when you want to enhance expansion and an exhalation when you want to enhance compression. Here are a few examples of how I implement my two training principles into exercise selection. Movement within each example can be supported or limited with changes in position, respiration, or execution.
1. Supine Reach
The supine position is combined with a bilateral arm reach forward with the intention to expand the upper thorax during inhalation. The position can also be used as a tool to teach stacking the thorax over the pelvis by cueing a hip tuck and soft exhale to move the front side of the ribcage downward. Our “stack” IS the set-up position for your main loaded, lift exercises (squat, deadlift, etc).
Check out how the inhalation expands the upper thorax and the exhalation creates compression.
Now you will not be able to take your eyes away from those two movement strategies.
2. Staggered Stance “Camporini” Deadlift
The staggered stance position is going to magnify the expansive capabilities of the lower, posterior hip of the back leg. The staggered stance position allows you to use the front leg to push back to the side of the back leg and align the pelvis and thorax back and to the side of the back leg.
The opposite arm reach allows you to transition the weight to the back leg. The expansive capabilities can be enhanced in the posterior hip with an inhale during the hip movement backwards (hinging).
3. Low Cable Step-Up
The staggered stance position puts the hip of the elevated leg in flexion (expansive) and the hip of the leg on the ground in an extension (compressive) biased position.
The addition of an opposite arm cable hold expands the backside of the upper back (avoid resisting the cable). The posterior hip of the elevated leg will compress as the individual pushes their foot into the ground and moves against gravity to perform the step-up.
At the bottom position, expansion can be enhanced in the posterior side of the flexed hip and posterior side of the arm holding the cable during an inhalation. Coaching cues may magnify expansion and compression within areas of the body by pairing respiration within phases of the exercise. Try inhaling at the bottom position and exhaling during the movement/step-up.
4. High Hip Reverse Bear Crawl
The bear crawl exercise is performed in a prone position. The additional component of the high hips and reverse direction promotes expansion in the upper thorax and posterior hips. You can coach continuous breathing through the movement or pause at certain points to inhale.
This is a fantastic warm-up exercise!
5. Tempo Squat Paired with Respiration
The squat starts in a standing position.
The assisted squat will also include a positional component of both arms reaching forward (same as goblet squat, zercher squat, or safety bar squat) which encourages the ‘stack’ position of the thorax and pelvis. The assisted squat is an example of turning positional breathing work into fitness. The squat movement requires both expansive and compressive capabilities within various phases of the movement in order to be able to descend and ascend against gravity.
The exercise can be used to teach people to change levels with a stacked, vertical torso. As a general notion, inhale down and exhale up.
6. Medicine Ball Lateral Stance Weight Shift Load and Release Throw
The exercise is performed in a lateral stance position.
Here, we are adding fitness with an emphasis on power, to positional breathing work!
Pair an inhalation with pulling the medicine ball across the body (transitioning weight from inside to outside leg) to bias expansion of the posterior hip of the outside leg. Then pair an exhalation with the throw to bias compression, exiting the hip of the outside leg.
This exercise also encourages rotational abilities and power through creating expansion and compression in specific areas of the body. For example, if you want to promote right rotation, you will need right anterior compression, right posterior expansion, left posterior compression and left anterior expansion abilities.
Conclusion
The use of positional breathing activities can improve our abilities to move with speed, free up range of motion at the shoulders and hips, rotate powerfully, and move up and down efficiently. My training principles are derived from this concept. My specific strategies are implemented through exercise selection, cueing, teaching, and pairing respiration with movement phases.
The ‘stacked’ position emphasizes a congruent relationship between the rib cage and pelvis (thoracic and pelvic diaphragm) and I believe it can serve as a foundational position to support movement. I want to thank Bill Hartman for exposing me to this lens of movement.
Implement these strategies with your clients and you’ll discover that positional breathing work WILL help your clients squat, hinge, run, rotate, and move better.
Principle Based Coaching
A strategy such as positional breathing work for better client movement is only as good as your ability to implement and communicate it with your clients. We become better at implementation and communication through analysis and development of our PRINCIPLES.
In this webinar, we will take a step back and learn the skills to formulate principles, make new information useful, AND IMPLEMENT information. At the end of the webinar you will know how training principles can be used to:
Make new information useful to YOU, YOUR clients, and YOUR business
Clarify your coaching decisions
Develop a more pinpointed coaching eye
Plan more effectively to get your client results
Gain confidence in your abilities and formulate your own coaching identity
If you have a shoulder (or two) chances are there’s been a time in your life where things haven’t felt great. This sentiment is only amplified if you happen to be someone who lives an active lifestyle playing sports and/or enjoys lifting heavy things.
There are a myriad of culprits that can lead to shoulder pain.15
One of the staple drills I like to use to accomplish the above (scapular upward rotation & protraction) is the Forearm Wall Slide.
Admittedly, it’s a simple looking thingamabobber of a drill.
I mean, all you do is move your arms up and down on a foam roller, right?
Weeeeeeeeeeeeeeeeeeee.
Alas, simple in appearance, not so simple in execution.
TOP VIDEO showcases two common faults I see when most people perform this drill.
❌ Reps 1-3 = depressed or “pinned down” scapula. Incessantly cueing your clients/athletes to retract & depress the shoulder blades has ramifications.
Sure, it’s an excellent cue to lift a metric shit ton of weight. There’s a reason why we tell people to bring their shoulder blades together and down during a bench press.
However, the scapula is meant to move around the ribcage and it’s imperative for overall shoulder health. When someone is pelted over the head with “together & down, together & down” cues the end result is a shoulder blade that’s cemented in a downwardly rotated position.
This can (not always) lead to shoulder ouchies.
❌ Reps 4-6 = shrugging pattern. The upper traps do play a significant role in shrugging (elevation). Shrugging, however, is NOT upward rotation.
In both scenarios there’s no “real” upward rotation happening.
The drill is ineffective.
Bye, Felicia.
BOTTOM VIDEO showcases what we actually want to see happen.
I like to cue people to “reach” towards the ceiling through their pinky finger, and then to sorta lean into the wall as the arm straightens overhead.
Here we get the upper trap to kick in more effectively and we can now see a shoulder blade that’s upwardly rotating (and moving around the rib cage via protraction & Serratus activation).
Performing with shirt off = 37% more Serratus Anterior activation. #science.
It’s crucial when choosing certain drills – even the seemingly simple looking ones – that they’re executed the right way. The details and nuances matter.