It’s not uncommon for people to seek out a coach or trainer because an exercise doesn’t feel right or because something – a shoulder, a knee, lower back, their soul perhaps – routinely hurts and they can’t seem to get out of their own way.
That’s where I come in to save the day.
Most of the time.
To fix someone’s squat technique and to maybe (probably) give him or her a reality check.
Boom or Bust
This is a term I stole from a friend of mine, Dan Pope of Champion Physical Therapy & Performance, and to a larger degree has its roots from a presentation I watched him do centered around the conversation of understanding shoulder pain.1
“Boom or Bust” refers to the person who handles their business as follows:
Train –> Do a lot –> To the point where it becomes painful –> Get pissed off, becomes upset, is inconsolable, and inevitably increase their volume of ice cream and Julia Roberts’ movies –> Feels better –> Repeat –> Cue face palm here.
I’m sure many of you reading – whether the above sequence of events describes you or some of your clients – can commiserate.
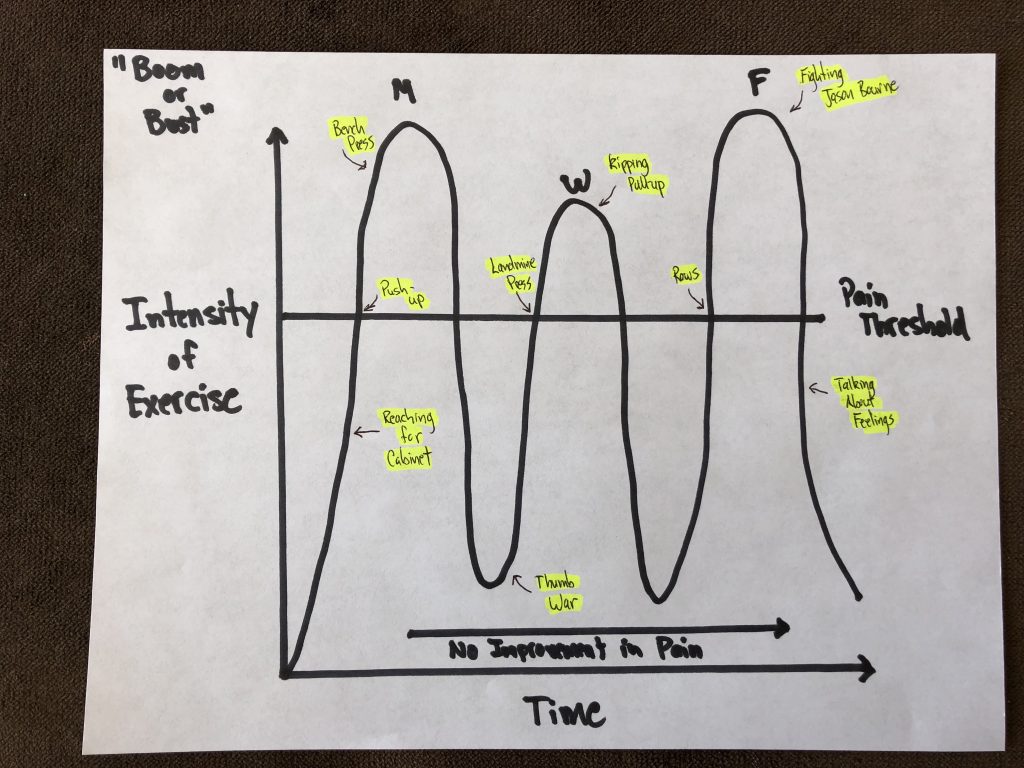
It can all be summarized using the following graph:
Again, props to Dan Pope. I essentially drew his graph, but added a little Tony LOLs.
What this depicts is a scenario and approach that keeps the alarm system sensitive as well as pain levels up. They train hard on Monday and hit their bench pretty aggressively, of course.
A day or two passes, the shoulder feels okay, and they decide to test the waters again and perform a bunch of high-rep push jerks. Another day or two passes, the shoulder starts to feel, normal again, and since they have zero fucks to give, decide it would be a swell idea to perform kipping pull-ups paired with handstand push-ups for AMRAP on broken glass.
All they do is perpetually plow through their pain threshold and the cycle continues over and over and over again like an episode of Russian Doll.
This, of course, is absurd, and makes zero sense.
Conversely, what also makes zero sense is the opposite approach…
…UNDER-loading, over corrective exercising people to death, or worse, doing nothing at all.
I’m not dissing the corrective component. Depending on how sensitive someone’s pain threshold is, we may very well have to resort to a myriad of side lying external rotations, arm-bars, and band work.
The key to improving pain, though, particularly with the long game in mind, is to elicit a smidge (key word: SMIDGE) of it during training. You want to tease it, buy it a drink, make out with it a little bit.
If you want to elicit change, you need to move. When we move, we induce something called mechanotransduction, which is just nerd speak for “tissue begins to heal.”
Pain, when DOSED ACCORDINGLY, can be beneficial during exercise. When we push into a little pain there’s generally better short-term results than if not. Think of it like this:
There’s a line in the graph above labeled “pain threshold.” On a scale of 1-10 (1 = no biggie, I got this and a 10 = holy shit, a panther just latched onto my carotid), exercise should hover in the 2-3 realm.
In this case, the person can tolerate things like push-up, landmine, and row variations.
When (s)he perform those exercises, the pain level never exceeds a “3.”
When (s)he’s done exercising, along with the hours after, the pain level never exceeds a “3.”
The following day, the pain never exceeds a “3,” and in an ideal situation is back down to baseline, which is a “1.”
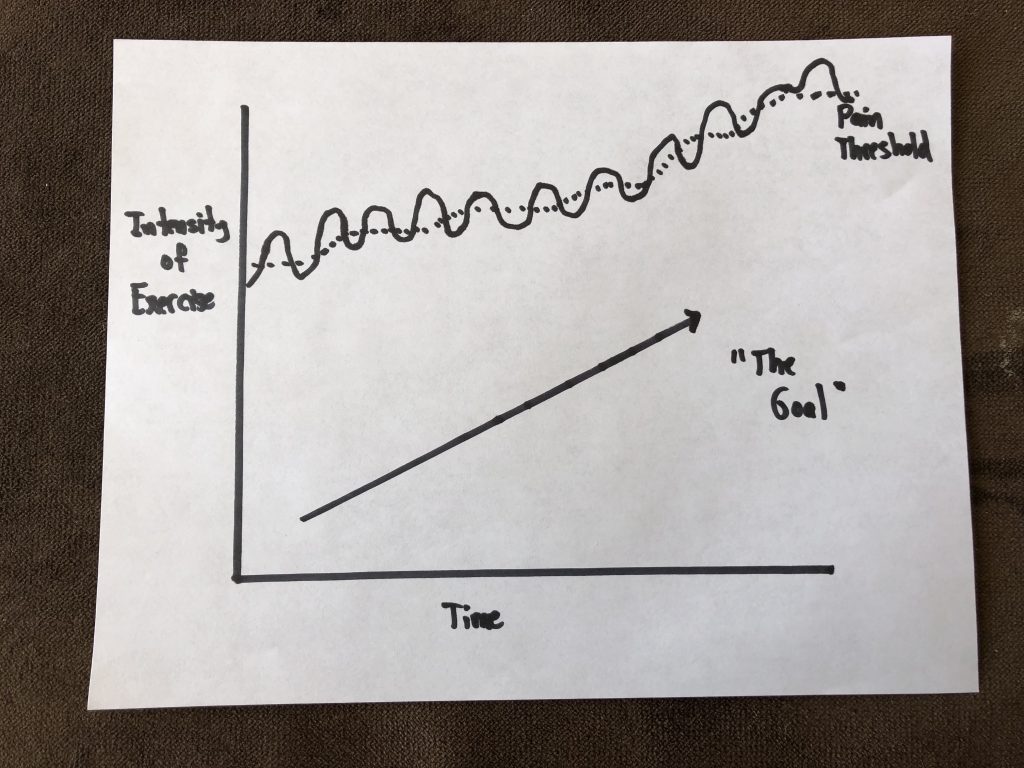
That’s the sweet spot and what we’re after from a managing pain standpoint. We’re doing juuuust enough to elicit a training effect, playing footsie with the pain threshold, but avoiding any boom or bust scenario where we place commonsense ahead of our ego.
And then, over time, the graph looks like this:
I’m an idiot. That arrow pointing up should be labeled “Improvement in Pain.”
The pain threshold slowly creeps higher and higher, and before long, push-jerks, bench pressing, and fighting Jason Bourne ain’t no thang.
Training (with weights), when matched with someone’s current ability level, and when dosed effectively, can be corrective.
Want More of These Awesome Insights?
Dean Somerset and I are reuniting after six years (thank you COVID) to bring our latest IN-PERSON workshop to the masses. The Complete Fit Pro Blueprint will cover topics like this (and many, many more).
Boston – June 6th-7th, 2026 Dublin, Ireland – October 3rd-4th, 2026
I remember when Julian was first born my wife and I had many, many “checklists” to make sure that our schedules were in line so that we knew who was doing what, and when to make sure that 1) Julian would be fed and 2) he’d get his naps in. We weren’t playing games with that shit.
It’s funny, though. It’s been a trip to see how I make connections and correlations between that and stuff I see and come across in my professional life… training and coaching athletes/clients.
One of the purest examples is something I witness on an almost weekly basis.
Many of the new people who start with me are beginner or intermediate level meatheads (male and female) who, for whatever reason(s), have been dealing with a pissed off shoulder that inhibits their ability to train at the level or intensity they’d like. It’s frustrating on their end and it’s my job as the coach to try to peel back the onion and see what may or may not be the root cause or causes.
That being said, I try not to go too deep down the rabbit hole. There’s a fine line between doing your due diligence as their coach and figuring out what may be causing their shoulder ouchies and making them feel like a patient.
READ: No one, and I mean NO ONE likes go to their personal training session and do rehab exercises for an hour. I’d surmise most would rather jump into a pool of lava. To that end, here’s my quick “go to checklist” whenever I have a client express that their shoulder hates them at the moment.
The “My Shoulder Hurts” Checklist
1) Technique
Most commonly people will note how bench pressing bothers their shoulder(s). Working on their technique is the baby check list equivalent of blow out explosive diarrhea.
I.e., It’s code mother-fucking red.
Following the mantra “if it causes pain, stop doing it” is never a bad call, and I am all for nixing any exercise or drill that does such a thing. However, I don’t like to jump to conclusions too too quickly. Sometimes making a few minor adjustments to someone’s technique or setup can make all the difference in the world.
Almost always I’ll have to spend some time on their set-up. I like to cue people to start in a bridge position to drive their upper traps into the bench and to set their scapulae (together AND down).
We can make arguments as to what this is actually doing. Some will gravitate towards it improving joint centration. Cool (and not wrong). I like to keep a little simpler and note that all it really does is improve stability.
A post shared by Tony Gentilcore (@tonygentilcore) on
Another thing to note is many people tend to flare their elbows out too much when they bench which leaves the shoulders out to dry and in a vulnerable position.
MINOR NOTE: Since recording that video above (many years ago), I have since changed my views slightly thanks to some cueing from Cressey Sports Performance coach Tony Bonvechio. Elbows tucked on the way down is still something I’m after (albeit some are too aggressive at the expense of placing too much valgus stress on the elbows). However, when initiating the press motion, in concert with leg drive, allowing the elbows to flare out a teeny tiny bit (in an effort to keep the joints stacked and to place the triceps in a more mechanical advantage) will often play huge dividends in performance.
In the end, much of the time it comes down to people not paying any attention to how crucial their set-up is. It’s amazing how often shoulder pain dissipates or disappears altogether with just a few minor adjustments.
2) What People Don’t Want to Hear: Stop Benching, Bro
This is where the Apocalypse begins. Telling a guy (usually not women, they could care less) that he should probably stop benching for the foreseeable future is analogous to telling a CrossFittter they can’t tell you they CrossFit.
The thing about holding a barbell is that it “locks” the glenohumeral joint into internal rotation which can be problematic for a lot of people and often feeds into impingement syndrome.
[The rotator cuff muscles become “impinged” due to a narrowing of the acromion space.]
NOTE: I hate the term “shoulder impingement” because it doesn’t really tell you anything. There are any number of reasons why someone may be impinged. Not to mention there are vast differences between External Impingement and Internal Impingement….which you can read about in more detail HERE.
If bench pressing hurts, and we’ve tried to address technique, I’ll often tell them to OMIT barbell pressing in lieu of using dumbbells instead. With DBs we can utilize a neutral grip, externally rotate the shoulders a bit more, and open up the acromion space.
Or, maybe they can still barbell press, albeit at a decline. When you place the torso at a decline the arms can’t go into as much shoulder flexion and you’re then able to avoid the “danger zone.”
If all else fails, sadly, you may have to be the bearer of bad news and tell someone that (s)he needs to stop benching for a few weeks to allow things to settle down.
3) Let the Scaps Move, Yo
Above I mentioned the importance to bringing the shoulder blades together and down in an effort to improve stability.
If you want to lift heavy shit, you need to learn to appreciate the importance of getting and maintaining tension. That said, if lifting heavy shit hurts your shit, we may need to take the opposite approach. Meaning: maybe we just need to get your shoulder blades moving.
When the scaps are “glued” together and unable to go through their normal ROM it can have ramifications with shoulder health. Push-ups are a wonderful anecdote here.
Unlike the bench press – an open-chain exercise – the push-up is a closed-chain exercise (hands don’t move) which lends itself to several advantages – namely scapular movement.
4) More Rows
This one will be short and sweet. Perform more rows. Many trainees tend to be very anterior dominant and spend an inordinate amount of time training their “mirror muscles” at the expense of ignoring their backside. This can lead to muscular imbalances and postural issues.
This makes me sad. And, when it happens, a kitten becomes homeless.
You sick bastard.
The easy fix is to follow this simple rule: For every pressing motion you put into your program, perform 2-3 ROWING movements. Any row, I don’t care.2
5) Address Scapular Positioning
I’m going to toss out an arbitrary number and I have no research to back this up, but 99% of the time when someone comes in complaining of rotator cuff or shoulder issues the culprit is usually faulty scapular mechanics. Sometimes people DO need a little more TLC and we may need to go down the “corrective exercise” rabbit hole.
The scapulae perform many tasks:
Upwardly and downwardly rotate
Externally and internally rotate
Anteriorly and posteriorly tilt.
AB and ADDuct (retract and protract).
Will clean and fold your laundry too!
They do a lot. And for a plethora of reasons, if they’re not moving optimally it can cause a shoulder ouchie. Sometimes people are too “shruggy” (upper trap dominant) with overhead movements, or maybe they’re stuck in downward rotation? Maybe they can’t protract enough and need more serratus work? Maybe they lack eccentric control and need a heavy dose of low trap correctives?
It dumbfounds me the number of times I have had people come in to see me explaining how they had been to this person and that person and NO ONE took the time to look at how their shoulder blades move.
I don’t like to get too corrective too soon, but if I’ve exhausted all of the above and stuff still hurts….it’s time to dig deeper.
If only there were a resource that dives into this topic in a more thorough fashion.
Full Disclosure: I am not a fantastic presser. I’m not going to sit here and attempt to regal you with stories from high-school where I used to drive a Camaro, hookup with the Prom Queen, and bench 405 for reps (you know, before that nasty football injury in the State Championship ruined everything).
Nope, this is not that kind of story. I recognize the bench press often serves as a litmus test for general level of badassery, but I’ve always considered myself an average presser (personal best of 315 lbs at a bodyweight of sexy).
Or, in Dave Tate’s words “I suck.”
Not gonna argue with Dave…;o)
I know how to coach it, and have worked with many people in my years as coach to help them improve and increase their bench press. More commonly, though, is helping people work around a nagging shoulder injury that prevents them from “attacking” the lift in the first place.
NEWSFLASH: Many people complain that the bench press bothers their shoulder.
And while the first inclination is to nix the bench press altogether and jump into corrective exercise mode and start having people blow into balloons or perform any number of thoracic mobility or scapular stability drills to get at the (possible) root of the problem, I feel we sometimes need to pump the brakes.
I mean, I agree that for many people their upper back mobility is atrocious and that it’s likely a very good use of their time to address it. And yes, some people may have gunky tissue quality or less than exemplary scapular stability or kinematics which likely is playing a significant role in their ouchie shoulder.
A thorough assessment or appointment with a manual therapist can hopefully help.
But maybe, just maybe, the reason why someone’s shoulder(s) hurt during bench pressing is because their technique makes my eyes bleed?
*shrugs*
Maybe all they need is a little more coaching. As I always say:
“Correct movement can be corrective.”
This is why, when someone’s shoulder hurts during the bench press, my first “tier” to attack is technique. The fitness industry has become too corrective at the expense of coaching our athletes/clients. Taking the 5-10 minutes to address someone’s set-up can make a huge difference in how the movement feels.
Are they driving their upper traps into the bench?
Are they getting their scapulae retracted and depressed?
Do they press the bar up and out of the j-hooks, or do they “guide” the bar out?
Do they “let the bar settle” before they lower it?
Do they “meet the bar with their chest? Or do they allow their shoulders to roll forward?
All of these can be easy-to-fix snafus that may eliminate any shoulder discomfort during the bench press.
Bench Press Set-Up
What happens if you address technique, it’s sound, and the bench press still hurts? You can still implement other pressing variations that can work in the interim while you address the root cause(s).
Decline Bench Press
Think about what’s not happening during a decline bench press as opposed to a flat or incline bench variation?
In a decline there’s less shoulder flexion involved which helps keep many trainees out of the “danger zone” of shoulder pain. So if flat bench pressing hurts you may be able to get away with a decline.
Spoto Press (Invisible Board Press)
A common flaw I see is some people have a hard time “meeting the bar with their chest” and end up having their shoulders roll forward as they lower the barbell.
Popularized by Bench Press Captain America, Eric Spoto (722 lbs, unequipped), the Spoto Press is a variation to combat this where you stop the bar a few inches above the chest, pause, and then press back up.
When In Doubt, Use Dumbbells
When you grab a barbell with a pronated (overhand) grip, you “lock” the humerus in an internally rotated position which can be problematic since it narrows the acromion space.
Using dumbbells alleviates this issue because you can nudge a little more external rotation by adopting a neutral grip. This is a major reason why I prefer DB pressing variations for overhead athletes as opposed to straight bar.
Corrective Pressing Variations That Don’t Feel Corrective
While not always the case, a common thread I see when it comes to shoulder pain is the INability of the shoulder scapulae to be able to move. In order to move big weight you need to respect tension and stability. In some cases, however, the shoulder blades are kinda “stuck” (usually downward rotation) and lack the ability to move through a full ROM.
It’s still vital to be able to access scapular movement for overall shoulder health.
When this happens I prefer to use pressing variations that allow for a little more wiggle room. As in: we allow the shoulder blades a little breathing room. Push-ups will always be my first choice here. But relax, I recognize most would rather swallow a live grenade than read more about push-ups.
For those interested you can READ this brief article.
Off-Bench DB Press
Scooting a smidge to the side of a bench will allow more scapular movement. What’s nice about this exercise is that it’s also a great core exercise (you have to fire like crazy in order to not fall off the bench) in addition to an awesome way to further engage the glutes. You can’t quite see it with the angle of this video, but I’m also situated further down on the bench so my lower half isn’t resting on it.
Bottoms-Up Press – Off Foam Roller
I snaked this one off Dr. Joel Seedman. Using a KB and holding it in the bottoms-up position is a fantastic way to ramp up rotator cuff activation…you really have to fight to stabilize and keep the joint centrated.
Moreover, by lying on the foam roller the shoulder blades are now able to move to a higher degree. And, much like the off-bench variation above, there’s also a high degree of glute engagement as well as foot and ankle engagement.
And That’s That
Don’t be so quick to bust out the band external rotations and t-spine drills. Addressing technique on the bench press can be every bit as corrective in terms of addressing shoulder pain. Likewise, don’t be so quick to omit all pressing variations. All aren’t equal and it oftentimes is a matter of choosing the right variation for the individual and nice vice versa.
We moved both courses to a new platform which will make both the delivery and user experience more enjoyable and seamless.
Dean and I both have a bunch of new followers4 since we last put them on sale.
It’s a new year and as such a lot of fitness professionals will need to start thinking about ramping up their continuing education and getting their CEU requirements in order.
Last but not least, we’re awesome.
Go HERE to enroll in one (or both courses).
IMPORTANT: use the coupon code wutang50 to receive your $50 off credit at checkout.
Now to the Shoulder Stuff
We can easily make the case that the shoulders are the most annoying and often injured part of the body for many people, meatheads in particular. And, to be candid, there are any number of things to consider with regards to why:
Rotator cuff weakness
Poor scapular stability (<– better term would be Controlled Scapular Mobility)
Postural considerations
Acromion type
Scapular kinematics (inability to upwardly rotate, for example)
It’s weird, though, when it comes to programming for the shoulders there’s this dichotomous yin-yang approach we have to consider:
What’s best for optimal (shoulder) performance?
And.
What’s best for optimal (shoulder) health?
Shoulder Performance
I’m in the business of helping people get bigger, faster, stronger, and generally more dieselfied.
This usually (but not always) revolves around lifting objects of appreciable weight. Watch any strong person bench press, squat, or deadlift a lot of weight and there’s a common theme you’ll notice:
1. You’ll likely have to unclench your sphincter after watching someone do something you never thought humanly possible:
2. With regards to the shoulders – specifically the shoulder blades – there’s meticulous attention paid to their positioning.
Those bad boys are locked down. Retracted and depressed.
Or, in non-geek speak: They’re not moving.
Doing so provides an infinite more amount of stability to the joint and also provides a more stable base of support (particularly for the bench press) to push from. When it comes to the deadlift and/or squat it allows one to maintain a more “rigid” torso, stay tight, and decreases the chance of energy leaks.
Force is more efficiently transferred within the kinetic chain.
Also, in non-geek speak: Just fucking trust me.
I’m no Eric Spoto, but I know how to coach the bench press and what to consider when it comes to performing at a high(er) level and making it so your shoulders don’t hate you.
Bench Press Set-Up: Shoulders Together & Down
Shoulder Health
It’s funny, when Dean Somerset and I teach our Complete Shoulder & Hip Blueprint workshop I’ll spend half a day imploring attendees to adopt the strategies mentioned above.
“Lock them down.”
…is what I’ll tell them. Referring to the shoulder blades and how it’s crucial to recognize ideal placement for performance
Then, after the lunch break, I’ll do a complete 180 and spend the rest of the day saying something to the effect of:
“Let those fuckers move.”
The shoulder blades do a lot:
Retract and protract
Elevate and depress
Upwardly and downwardly rotate
Posteriorly and anteriorly tilt.
It’s imperative to have “access” to the full spectrum of scapular motion in order to obtain optimal shoulder health.
We spend so much time telling people to squeeze their shoulder blades together – which, all told, isn’t a bad cue in of itself, but can cause a whole host of shoulder ouchies; downward rotation syndrome for starters – that it’s no wonder I get a range of quizzical looks whenever I tell people to let them move.
Protraction (or reaching) is a game changer for many.
1-Arm Quadruped Protraction
Easy Scapular Winging “Fix”
To go a step further and outside the “corrective” realm, when I coach people through a push-up or any kind of row variation a common mistake I find people make is keeping their shoulder blades pinned or glued together.
With push-ups I try to tell my clients to push away or “finish” at the top.
I don’t want their shoulder blades making out the entire time.
And with rows…
This Makes Me Sad
You’ll notice my shoulder blade isn’t moving at all; it’s staying in the retracted position throughout the duration of the set. This often leads to bicep tendon issues and anterior shoulder instability, amongst other things.
Instead I try to tell people I want their scapulae to move around their rib cage. After all that’s what they’re meant to do.
That’s More Like It
It’s profound how much this seemingly minor tweak will help with a lot of shoulder woes.
That’s It
Pretty easy, right?
Short, precise, and won’t require a book report.
Making a concerted effort to recognize and address both ends of the shoulder performance-health spectrum can and will make a huge difference and help you write more effective programs.
Needless to say: 1) I have a potty mouth (#sorrynotsorry) and 2) I’m a firm believer that strength training is not only a wonderful (and often overlooked) way to get people strong(er) – duh! – but also as a means to “correct” or address a perceived dysfunction/road block in movement.6
I work with a lot of individuals who complain of shoulder ouchies, especially as it relates to performing stuff overhead.
There are any number of factors to consider:
Tight lats.
Poor anterior core strength.
Tight pecs.
Wearing blue.
Who knows? Lots of things can run awry.
I think it behooves any coach/trainer to put on their detective’s hat, dig deep(er), and try to ascertain what could be the root cause for someone’s discomfort or pain.
SIDE NOTE: Too, I think it’s important to be careful of scope of practice and not DIAGNOSE anything. Nothing irritates me more – other than people who refer to themselves as an “entrepreneur” or “influencer” – than a personal trainer who thinks he or she is a physical therapist or doctor and attempts to diagnose their clients:
“Ah, yes, I see your left shoulder lacks internal rotation. I think it may be cancer.”
It’s within our wheelhouse to assess movement, of course, and to use that information to help guide programming. But outside of that I implore you to stay within your lane and not get into the habit of diagnosing anything.
Okay, end rant.
Back to why someone’s shoulder hurts.
All of what I mentioned above applies and can definitely be a part of the conversation.
One factor, however, that often gets glanced over is the congruency of the shoulder blades and rib cage.
I.e., Can a concave scapula play nicely together with a convex rib cage?
One way to accomplish this is to give the Serratus Anterior muscle waaaaaaay more attention than we typically give it. The Serratus is a “reaching” muscle and helps the shoulder blade move AROUND the rib cage.
For those who have been incessantly told to keep the shoulder blades “together & back” – which, to be fair, is important to lift heavy things – it can sometimes result in faulty mechanics where they’re more or less cemented in place.
And, shoulder blades that don’t move = no bueno.
Renowned physical therapist, Shirley Sahrmann, popularized the phrase “Scapular Downward Rotation Syndrome” in her book Diagnoses and Treatment of Movement Impairment Syndromes.
Without getting into the wordplay too much, Downward Rotation Syndrome can be the result of a few things, but the main players at play are (generally) overactive/tight Rhomboids, levator scapula, and lats. Symptoms can range anywhere from subsequent glenohumeral compensatory joint motion (joint fraying to tears) and instability to neck pain, and, in extreme cases, thoracic outlet syndrome.
It sounds like some nefarious, end-of-days stuff (and it can be).
However, rest assured the “fix” can be quite accessible.
Anything which allows more reaching (protraction), in addition to better access to rib cage expansion (movement), can be MONEY for many people.
You can see both in action in what’s undoubtedly the most boring video on the internet.
1️⃣ As I press my hands forward I’m thinking about reaching as far out in front of me as possible (I’m not keeping the shoulder blades still).
Hello Serratus. Nice to meet you.
2️⃣ As I progress overhead I’m reaching upward towards the ceiling with my upper traps, staying careful not to cheat via my lower back. Ribs stay down.
Not coincidentally BOTH – Serratus & Upper Traps – play an integral role in scapular upward rotation.
The shoulder blades are designed to move!
If overhead activities hurt it could be because you’ve programmed yourself to keep them in place.
3️⃣ At the top I’m OWNING the position (very important) by adding a breath: INHALE through the nose expanding the rib cage all around. Then a FULL, accentuated, EXHALE to get the ribs down and promote a canister position (rib cage stacked over pelvis).
It’s harder than it looks.
4️⃣ Pants optional.
If you want to aid better overhead motion – or just help people’s shoulders feel better – it’s imperative to get the shoulder blades and ribcage to become BFFs and to OWN better position(s).
Less band external rotation drills and more Serratus activation in concert with positional breathing.
Just to help calm the waters: I am not anti “corrective exercise.”
And I am not really going to throw my face into a brick wall.
I respect and can appreciate that, sometimes, our jobs as fitness professionals require us to pump the brakes and to venture down the corrective exercise rabbit hole.
Some people require a bit more TLC with regards to improved movement, motor control, and/or, and I’m paraphrasing here…”just learning to turn shit on.”
Some people will require a laundry list of additional mobility work, stretching, or positional breathing drills to point them in the right direction and to help them feel better.
What I am against, though, and what drives me bonkers, is when coaches and personal trainers go out of their way to:
1) Overstep their scope of practice and end up performing really shitty physical therapy with their clients and athletes.7
OR
2) Highlight every minor “dysfunction” with a client/athlete – excessive anterior pelvic tilt, kyphotic posture, left eye is lower than the right (you freak) – making him or her feel as if they’re walking ball of fail.
Here’s another gleaming example of how TRAINING is corrective and how, if we do our jobs as coaches, we can often accomplish a lot sans the brick wall.
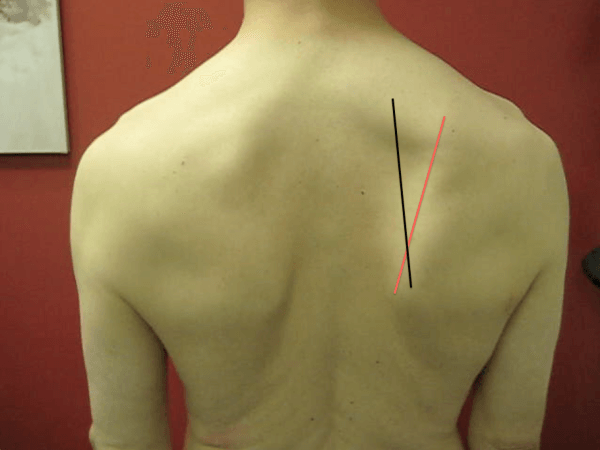
My client, Emily, who’s a trainer herself, has been dealing with some left shoulder issues. I had her come in the other night to see if I could offer some insights and to listen to some sick EDM beats.
The latter has nothing to do with anything, but whatever….give THIS a listen.
Emily showed up and I took the picture below. It shows something clearly awry and that some sort of shoulder clusterfuckey was at play; namely lack of shoulder flexion on the left side.
What was the culprit?
It could have been a few things:
Capsular issue
Lack of scapular rotation (namely upward rotation).
Soft tissue restriction.
Lack of lumbo-pelvic control.
It was a Wednesday.
I don’t know.
What I do know is that I had to respect my lane and understand it wasn’t my job as a strength & conditioning coach to diagnose anything.
I could, however, assess her general movement capacity, use my knowledge of anatomy, and perform a little trial and error to see if I could improve things.
What follows is more or less a brain dump and an attempt to explain my thought process as I worked with Emily for the next hour.
I’m not gonna say that what ended up happening was on par with some Matrix level shit, but I will say I basically know Kung-Fu.
“What actions have to happen at the scapulae in order to get the arms overhead?”
– Upward rotation
– Protraction
– Posterior tilt
Emily wasn’t getting much upward rotation on that left side. When I asked her to bring her arms overhead it was as if her left arm hit a massive speed bump and came to an abrupt stop. She could push through it, but not without pain.
So I had to think about what muscles help with that action (upward rotation)?
– Upper and lower traps
– Serratus
Too, I noticed she also had a more depressed shoulder girdle as a whole; her clavicular angle was more horizontal rather than having a slight upward grade.
HERE‘s Eric Cressey discussing this in a little more detail.
I surmised her UPPER traps needed some attention.
The upper traps often get a bad rap and are avoided like a Coldplay concert. In certain populations (think: desk workers) and instances, the upper traps are OVERactive and can play a role in increased shoulder elevation as well as superior migration of the humeral head, and hence an increased risk for shoulder impingement.
In this scenario, it behooves us to not go out of our way to increase upper trap activation.
However, we often forget the upper traps are a major player in UPWARD ROTATION, not to mention help with scapular elevation…both of which, in my eyes, Emily could have used some more of.I didn’t get over corrective with Emily and start having her perform some voodoo like tapping her pinky finger three times while flossing her teeth with a strain of hair from a Hippogriff.
I didn’t have her perform a laundry list of “correctives” that, for all intents and purposes, would have likely made her feel like a patient and bore her to tears.
Nope, I had her TRAIN and just modified a few things.
We did:
1. Landmine Presses with a Shrug/Reach
2. Face Pulls in an upwardly rotated position (so the upper traps were more engaged)
3. And, instead of performing movements that would pull her into more shoulder depression and downward rotation (deadlifts, farmer carries, etc) we opted for Landmine Squats, Zercher RDLs, and Hip Thrusts.
In short: We turned shit on (upper traps) and trained movements that (likely) wouldn’t feed into the root causes of her symptoms.
Here’s the picture I took at the end of her session:
Anyone who’s spent any significant time in the weight room knows how vulnerable the shoulders are to injury.
This isn’t to downplay other areas of the body prone to nefariousness like the lower back or knees. Let’s be clear: those deserve some shade thrown their way too.
Rather, it’s just to point out that, for lack of a better term, trying to train around or even fix a pissed off shoulder sucks donkey balls.
It can be tricky and there are a lot of factors to consider: Exercise selection, exercise technique, posture, access to appropriate scapular motion (upward vs. downward rotation), soft tissue considerations, and breathing patterns to name a few.
Taking all of the above into consideration is a good thing, and I applaud those coaches and trainers who go out of their way to peel back the onion as much as their expertise and experience allows in order to get at the crux of the issue.
I do find, though, that sometimes, not always, we get a little too cute or rabbitholey with our approach to shoulder health.
Coach A will tell one individual that their shoulder hurts because their left big toe lacks dorsiflexion.
Coach B tells them it’s because their Posterior Mediastinum is shutting off their diaphragm.
Coach C says “nope, your shoulder hurts because you’re not back squatting enough.”
And Coach D, well, he’ll say something really asinine like, “I think it’s because you’re wearing purple. This makes your shoulder sad.”
And yes, while I am being a tad facetious here, I don’t feel I’m coming entirely out of left field. I’ve heard some doozies from past and current clients about what they were told was the impetus behind their shoulder woes.
Moreover, as a result, many clients and trainers alike tend to fall under the same trap….
….OverCorrectiveExerciseitis
This falls under two camps:
Camp 1: Trainer gives or person is handed a laundry list of “corrective exercises” that take 327 days to complete.
Camp 2: Trainer prescribes or person is told to perform redundant, borderline stupid exercises.
Stop OverCorrectiveExerciseitis
All of this isn’t to say I’m anti “corrective exercise” or that it should be avoided altogether. There’s a time and place for just about everything8, and sometimes people do need a little bit more TLC to improve motor control, activation, and/or positioning.
PSA: Doing stuff correctly can be corrective. Avoiding excessive anterior humeral glide during push-ups or rows can be a game changer for shoulder health.
However, Dr. Quinn Henoch brought up a valid point when I listened to him speak a few months ago with respects to corrective exercise.
Maybe the real fix for most trainees is something as simple as adjusting their training volume.
Maybe they’re doing too much of one thing or too little of another?
Generally speaking, when someone’s shoulder hurts I find most need less bench pressing and more posterior cuff and upper back strength in addition to a healthy dose of scapular stability.
Instead of boring them to tears with warm-up drills they’re likely not going to do on their own anyways, I prefer to include the bulk of the “correctivy” stuff IN THEIR ACTUAL PROGRAM.
That way they just think it’s business as usual and I come across as a straight up boss for helping them cure their shoulder woes.
On Bench Pressing:
There’s lots more to say here, and this will likely make for a good blog post in the future, but in the interim the Tweet below sums things up succinctly:
Bench press hurts your shoulder checklist/hierarchy: 1) audit setup/technique, 2) adjust volume, 3) grip…the…bar….harder, 4) corrective considerations, 5) maybe not bench press? (with a straight bar).
Below are two drills I like to use as fillers that can be performed after sets of squats, deadlifts, and even bench presses. It’s a foolproof way to add more volume to something they’re probably not doing enough of anyways.
It’ll look something like this:
A1. Deadlift/Squat/Bench Pressing/Not Kipping Pull-Ups A2. Filler (<— correctivy stuff that people just think is part of their program so they actually do it. Hahahahahahahaha. Jokes on them).
As you walk back you need to resist the pull of the band, which torches the rhomboids, muscles of posterior cuff, and scap stabilizers. Be careful you don’t “shrug” throughout, you want to keep shoulder blades depressed and together.
NOTE: 118% more effective if you yell “this….is….Sparta” as you perform your set.
I like to have my clients perform anywhere from 5-10 reps per set.
2. Racked ISO Shoulder Holds
This is another drill I stole from someone smarter than myself, this time a Doctor: Dr. Ryan DeBell of The Movement Fix.
I’ll usually start with 10 second holds at each position per set and ramp up to 20-30s holds per set for my clients (depending on how sadistic I feel).
I’ve seen some very big individuals succumb to this drill. It’s very humbling.
That’s It
Pepper these two drills into your workouts or that of your clients/athletes more sporadically. I’m certain everyone’s shoulders will start feeling better.
Bicep Tendonitis? When In Doubt Check These 5 Muscles Out
Knowledge and wisdom are not one in the same. A profound statement for an article that is going to discuss pain at the plain old bicep tendon. The reason I bring this up is because an endless amount of information is available to you through the internet.
When you search bicep tendon pain you will likely run into 100,000 articles that talk about pain local to the bicep tendon. I could make an argument that less than 1% will discuss techniques that you can implement to independently resolve your pain.
That is our plan for today.
Before we start drawing up a six week rehabilitation plan for your shoulder or sending you to the nearest orthopedic surgeon, lets attempt some quick fixes. Please, do not mistake a quick fix with a half-hearted attempt.
Refrain from replacing the whole roof when a few shingles will do.
Step one is making sure you are an appropriate candidate for this article. Let’s rule out a bicep tendon rupture!
Schedule an appointment immediately with an Orthopedic Physician if:
1. You heard a sudden “ pop” at the shoulder, along with swelling and bruising around the bicep.
This typically occurs when you are trying to “man up” and carry something that is a tad bit too heavy for you. Often a result of your best friend refusing to pay for a moving company.
2. You have a nice “Popeye” deformity at the bicep.
This doesn’t imply that you have impressive biceps. It means you tore the bicep tendon.
Other Reasons For Concern:
Weakness and pain local to the bicep when flexing the bicep or rotating your palm up to the sky with the elbow partially bent. This does not indicate a rupture, but a partial tear is still possible.
I don’t think I tore my bicep tendon. What else could cause irritation to the bicep tendon?
It is common for the bicep tendon to be a pain generator because of its location. The bicep tendon is often impinged between the humerus and surrounding structures in the shoulder (usually the acromion and the coracoid process).
Keep in mind that impingement is normal.
We have nice “cushions” named bursae that are built to tolerate this compression. It is when this compression becomes too frequent or too intense that we see injury occur at the bicep tendon. We tend to see this in people who perform a lot of overhead activities in athletics or with work requirements.
It hurts when I rub my fingers across the bicep tendon. Doesn’t this mean it is a bicep tendon problem?
Simply rubbing your finger across the bicep tendon is not an accurate way to diagnose a bicep tendon injury. This is the most common mistake I see by medical providers and those with a certification in WebMD browsing. This is not a specific or sensitive test for diagnosing a bicep tendon injury. (Gill, HS)
What is the best way to determine if the bicep tendon sustained an injury?
The gold standard would be an ultrasoundfrom a physician (Skendzel, JG). Isolating the bicep is the next best method. Resistance to the bicep, or lowering yourself in a reverse grip pull up is also useful information.
It is possible that you have developed some inflammation local to the bicep tendon. Most of the special tests specific to the bicep do not have great statistics. We can make a more accurate diagnosis by considering how you sustained your injury and the movements that provoke your pain.
Could pain at the front of my shoulder be related to something else besides the bicep tendon?
Absolutely. Muscles throughout the shoulder and neck can refer pain to the front of the shoulder. The same way that organs can refer pain to different regions of the body.
Let’s check out 5 muscles that commonly refer pain to the front of the shoulder.
Note From TG: A lacrosse or tennis ball work well for all the drills demonstrated in the video, but my preferred “tool” is the ACUMobility Ball by ACUMobility.com.
Use the coupon code GENTILCORE at checkout for an additional 10% off your purchase.
Deltoid
People often forget that the muscle fibers of the deltoid run over the bicep tendon. When you feel pain while pressing around the bicep tendon it may actually be an irritated deltoid.
Biceps
Another no brainer if you are having pain around the bicep tendon. Overuse of the biceps or a quick force applied to the biceps (eccentric force) can cause trigger points to develop in this muscle. If you notice increased discomfort around the bicep some soft tissue work and a few days off from the “gun show” should help.
Pectorals/Subclavius
The real problem here could be too many chest days and not enough leg days!
Poor resting posture during the day and poor technique with exercise are often the true culprits. Falling into a slumped position on a regular basis can put the pectorals in a shortened position.
This faulty posture can lead to excessive impingement, as well as increased tone and trigger points in the pectoral muscles.
The subclavius runs deep to the pecs. It attaches between the clavicle and the first rib, often referring pain to the front of the shoulder. You can usually address this spot while working on the upper fibers of the pecs.
Scalenes
These muscles run on the front, side and back portion of your neck.
The scalenes are one of the many muscles responsible for moving your neck. If you tend to adopt a forward head posture or a slight tilt of the head to the left or right these muscles may be engaged more often than necessary.
Having a forward head posture means that you are passively hanging on these muscles for support during the day. This can lead to increased tone and trigger points. We also tend to see issues in the scalenes show up following a whiplash injury.
The scalenes are also involved in breathing. If you tend to be an upper chest breather these muscles may be taking a beating. Keep in mind, adopting this breathing style can lead to increased tension in the neck and thorax, as well as feelings of anxiety. After you do some soft tissue work, be sure to be more aware of posture and work on accessing your diaphragm.
Infraspinatus
The infraspinatus in one of the four infamous rotator cuff muscles.
It runs right on top of your shoulder blade.
Dysfunction in this muscle tends to show up regularly with shoulder pain. Trigger points in the infraspinatus are a problem because they alter timing and strength of this muscle (or any muscle). This alters normal mechanics at the shoulder with overhead activities. Often leading to an unstable shoulder with excessive impingement taking place.
We wrote another article in the past that discussed how referred infraspinatus pain also resembles carpal tunnel syndrome. This is not the easiest muscle to treat on your own, but don’t skim over it.
Final Consideration:
In some instances, performing soft tissue work around the shoulder will do the job just fine. This does not mean we can overlook the pieces that may have contributed to this injury in the first place. Your goal is to control what you have the ability to control.
What can you control?
1. You can normalize the tissues surrounding the shoulder.
Treat local trigger points, normalize muscle flexibility and reduce stiffness. The goal is to restore normal shoulder mechanics to the best of your ability. Treating muscle stiffness and trigger points helps optimize the timing and strength of the muscles around the shoulder to enhance stability.
2. You can also modify your activity for the time being.
If a certain activity worsens your pain, back off. It is possible that your shoulder is inflamed and needs some time to recover. This is not a fast pass to weeks off from the gym with your best friend Netflix. This means more attention on soft tissue work and flexibility. You also want to gradually return to exercise. Experiencing some discomfort during exercise is ok.
“Poke the bear, but don’t take it to dinner.”(in reference to pain)
– Adriaan Louw
Interested in a FREE Mobility Program to treat pain at the front of the shoulder? Click here
About the Author
Dr. Michael Infantino is a physical therapist. He works with active military members in the DMV region. You can find more articles by Michael at RehabRenegade.com.
References
Gill HS, El Rassi G, Bahk MS, et al. Physical examination for partial tears of the biceps tendon. Am J Sports Med 2007; 35:1334.
Skendzel JG, Jacobson JA, Carpenter JE, Miller BS. Long head of biceps brachii tendon evaluation: accuracy of preoperative ultrasound. AJR Am J Roentgenol 2011; 197:942.
Stephen M Simons, MD, FACSM, J Bryan Dixon, MD Section, Biceps tendinopathy and tendon rupture
Uptodate.com
Taylor SA, O’Brien SJ. Clinically Relevant Anatomy and Biomechanics of the Proximal Biceps. Clin Sports Med 2016; 35:1.
If you’re a human being reading this blog post it’s a safe bet you 1) have impeccable taste with regards to the strength coaches you choose to follow 2) have a pair of shoulders and 3) are likely interested in keeping them healthy and thus performing at a high level in the weight room.
NOTE: If you happened to have come across this blog post by Googling the terms “world’s best tickle fighter” or “The Notebook spoilers”….welcome!
I’m a little biased given my years of experience working with overhead athletes and meatheads alike, but I’d garner a guess that nothing is more annoying or derails progress more than a pissed off shoulder…or shoulders.
My friends Dan Pope and Dave Tilley of Champion Physical Therapy & Performance just released a stellar resource, Peak Shoulder Performance, that’s perfect for any coach or personal trainer looking to help their clients/athletes nip their shoulder woes in the bud. AND it’s on sale for this week only at $100 off the regular price.
Guess what most people think is the cause of their shoulder woes?
The rotator cuff.
Guess what’s likely not the cause of their shoulder woes?
The rotator cuff.
It’s lost on a lot of people that the “shoulder” isn’t just the rotator cuff.
I mean, N’Sync back in the wasn’t just Justin Timberlake, right?
JC, Lance, Chris, and Joey (<— didn’t have to look up all their names) deserve our respect and admiration too. They all played key role(s) as individual entertainers to make the group more cohesive, successful, and relevant.
The phrase “the whole is greater than the sum of its parts” has never rang more true than right here and right now, reminiscing on long past their prime 90’s boy bands.
[Except, you know, we all know Justin was/is the only one with talent. He can sing, he can dance, he can act, he’s got comedic timing. He’s a delight.]
The rotator cuff is Justin Timberlake.
It gets all the credit and accolades and attention with regards to shoulder health and function. However, the shoulder consists of four articulations that comprise the entire shoulder girdle:
Glenohumeral Joint (rotator cuff) – Justin
Acromioclavicular Joint – JC
Sternoclavicular Joint – Lance
Scapulothoracic Joint – Joey and Chris
I’d make the case, and this is an arbitrary number I’m tossing out here (so don’t quote me on Twitter), that 80% of the shoulder issues most people encounter can be pin pointed to the Scapulothoracic area (shoulder blades) and what it is or isn’t doing.
The shoulder blades, since you have two of them, are Joey and Chris.
Think about it:
Justin, JC, and Lance were generally considered the heartthrobs of the group and were always taking center stage, in the forefront, and amassing Tiger Beat covers.
Conversely, who was in the shadows, taking a back seat, presumably doing all the heavy labor, regional Mall appearances, and B-list talk shows the other guys didn’t want to do?
That’s right…..Joey Fatone and motherfucking Chris Fitzpatrick, son!
Lets Give the Scaps Some Love
All of this isn’t to insinuate the rotator cuff alone is never the culprit or that pain in that area should be shrugged off, ignored, and not addressed directly.
However, when lumping shoulder pain and the rotator cuff into the same sentence we’re often referring to something called “shoulder impingement.”
Shoulder impingement is a thing – loosely defined: it’s compression of the rotator cuff (usually the supraspinatus) by the undersurface of the acromion – and it is a nuisance.
There’s even varying types of shoulder impingement – Internal vs. External Impingement. Moreover, just saying “shoulder impingement” doesn’t say anything as to it’s root cause.
Many factors come into play:
Exercise Technique
Poor Programming
Lack of T-Spine Mobility
Fatigue (rotator cuff fatigue = superior migration of humeral head)
Faulty Breathing Patterns
Wearing White Past Labor Day
And Scapular Dyskinesis…to name a few
Just saying someone has “shoulder impingement” and telling him or her to perform band external rotation drills (oftentimes poorly) till they’re blue in the face doesn’t solve WHY it may be happening in the first place.
Often, the rotator cuff hurts or isn’t functioning optimally because something nefarious is happening elsewhere.
And on that note I’d like to point your attention to the shoulder blades.
Release, Access, Train
I have a lot of people/athletes stop by CORE because their shoulder(s) don’t feel great. Many have gone to several physical therapists prior to seeing me frustrated they’re not seeing progress, and if they are it’s often fleeting.
Full Disclosure: I know my scope and am never diagnosing anyone or anything.
Actually, Things I Can Diagnose = poor deadlift technique, poor movement in general, and epic poops vs. average poops (#dadlife).
Things I Can’t Diagnose = MRIs, musculoskeletal injuries/limitations, gonorrhea.
I find it amazing, though, whenever I do work with someone with shoulder pain, how much of a rare occurrence it is anyone ever took the time to assess scapular function.
If the scapulae are in a bad position to begin with (maybe in excessive anterior tilt or downwardly rotated) and/or are unable to move in all their glory (upward/downward rotation, anterior/posterior tilt, adduction/abduction, elevation/depression), or altogether move poorly…is it any wonder then, why, possibly, maybe, the rotator cuff is pissed off?
Photo Credit: EricCressey.com
While not an exhaustive list or explanation – everyone’s their own unique special snowflake – the following approach covers most people’s bases:
Release
Scapular position is at the mercy of the thorax and T-Spine.
Those in a more kyphotic posture – think: computer guy – will tend to be (not always) more anteriorly tilted and abducted.
Those in a more extended posture – think: athletes/meatheads – will tend to be (not always) more downwardly rotated and adducted.
In both cases the congruency of the shoulder blade(s) and thorax is compromised often resulting in an ouchie.
“Releasing” the area is often beneficial:
Access
Now that the area is released we can then gain “access” to improved scapular movement by nudging the ribcage/thorax to move via some dedicated positional breathing drills.
Think of it this way: if the ribs/thorax are unable to move because they’re glued in place, how the heck are the scapulae going to move?9
A few of my favorites include:
NOTE: Which one you use will depend on an individual’s presentation. A good rule of thumb to follow would be for those in a more extended posture to include breathing drills that place them in flexion and vice versa. There are always exceptions to the rule, but for the sake of brevity it’s a decent rule to follow.
All 4s Belly Breathing
The Bear
Supine 90/90 Belly Breathing
Prone Sphinx
NOTE: I didn’t discuss it in this video but I’d also encourage people to include a full inhale/exhale with each “reach” or repetition on this exercise.
Train (and Go Lift Heavy Things)
Now that we’ve released and gained access to the area, we need to train. Specifically, almost always, we need to improve one’s ability to move their arms overhead (shoulder flexion) without any major compensations.
In order to do so, the scapulae need to do three things:
Posterior tilt
Upward rotation (which, as a whole, describes the end goal)
Protract
All three entail utilizing the force couples of the upper/lower traps and serratus anterior in concert to help move the shoulder blades into the upwardly rotated position we’re after.
There are a litany of drills and exercises that can be discussed here, and it’s important to perform a thorough screen/assessment to ascertain which ones need to be prioritized.
Forgive the aloof and standoffish tone. I recognize the term “scapular winging” is a thing and that it can be an actual, real-live, medical diagnosis with dastardly consequences.10
But more on that in a minute.
It’s just that, in some ways, I find a lot of fitness pros – personal trainers, strength coaches, and even physical therapists – can often be a little too liberal with use of the term. They toss it around with little understanding of what it actually means and with little “feel” on how it’s interpreted by their clients and athletes.
I’ve long championed the sentiment that most (not all) fitness pros use the initial assessment as an opportunity to showcase how much people suck at doing things and how broken they are, and that, for the mere cost of a 215 pack of training sessions (the equivalent of a really, really nice Audi), they’ll fix you.
Pffffft, who wants an Audi anyways?
Here’s how a typical conversation goes:
Client: “Hey, I’m thinking about hiring someone to train me.”
Douchy Trainer: “Great, I’d be glad to help. We need to start with an assessment so I have ample opportunity to showcase how much of walking ball of fail you are and how I alone can fix you.”
Client: “Uh, okay. When do we start?
Douchy Trainer: “Right now, take off your shirt.”
Client: “Not going to buy me dinner first, huh? Kidding, okay, BAM.”
[takes off shirt]
Douchy Trainer: “Oh……….MY………..GOD.”
Client: “What? What’s wrong?”
Douchy Trainer: “I’m sorry to have to tell you this, but, you may want to sit down for this.”
Client: “Okay. What is it?
Douchy Trainer: “I’m sorry to have to tell you, but, but…..you have scapular winging.”
Client: “Is….that bad?”
Douchy Trainer: “I honestly have no idea how you’re able to walk, let alone speak complete sentences. We need to fix this ASAP.”
And this is where the trainer turns into that a-hole nun from Game of Thrones walking the client, Cersei style, down to the training floor to take them through a bevy of corrective exercise drills.
Now, admittedly, the key words used to find this picture were “most fucked up, dumpster fire of a case of scapular winging on the internet,” so don’t get too alarmed.
This is a legit, medically diagnosedcase, and not at all normal.
In a general sense, when we say “scapular winging” all we’re saying is that the shoulder blade comes or “wings” off the ribcage.
It’s sorta tricky because this pretty much describes everyone. You, me, George Clooney, your second cousin’s brother-in-law’s nephew’s Little League coach, literally, everyone, has some form of scapular winging.
So, what is it then? How much is too much? And, more importantly, what, if anything, should we do to fix it? Do we even need to fix it?
Dr. Quinn Henoch of Juggernaut Training Systems described this beautifully not too long ago. In short: a true case of scapular winging, like what’s pictured above, is a neurological condition where the Long Thoracic Nerve isn’t doing it’s job of innervating the Serratus Anterior (who’s job it is to adhere the shoulder blade to the ribcage).
The approach or fix in this case hasn’t anything to do with turning on “x” muscle or performing x, y, and z corrective exercises.
It’s not quite that simple.
Scapular Winging: What It Isn’t
I’ll tell you this much: we don’t have a pandemic of people walking around with true scapular winging. The vast majority of people you’ll encounter are owner’s of a completely healthy Long Thoracic Nerve.
They’re not broken. There’s nothing super duper nefarious happening.
What’s likely the culprit is a lack of tension and motor control.
The fix, then, is……..Drum roll…..
LOAD
If we can figure out ways to introduce load and subsequently, tension, this will not only help to turn shit on (without having to go down the 19-part corrective exercise rabbit hole) but also help people get into better positions via a little introduction to protraction.
Want to “cure” someone’s scapular winging in a matter of seconds?
Watch this. Closed-chain movements, protraction in general, is kind of magical.
Wall Press & Push-Ups That Don’t Suck
Pretty cool, right? That’s some Gandalf shit right there.
Quadruped Rockback w/ Floor Press
Typically the Quadruped Rockback is a a screen used to gauge active hip flexion ROM and to ascertain someone’s appropriate squat depth based of his or her’s anatomy. However, after listening to Mike Reinold speak on the topic it’s also a great drill to cue people into more protraction and upward rotation
Floor Press w/ Upward Rotation
Taking the floor press a step further, we can take away a base of support (and force the stabilizing arm to work that much harder in order to maintain position) and then incorporate some upward rotation.
Wrap Up
The umbrella theme here is not to dismiss scapular winging as an actual diagnosis. It is a diagnosis. It’s just not as common as people think, and I wish more fitness pros would stop jumping to conclusions so fast.
Oftentimes the fix is just to coach people up, introduce some load, and get them into better positions.
Last Chance to Save $100 off Complete Shoulder & Hip Blueprint















 Dr. Michael Infantino is a physical therapist. He works with active military members in the DMV region. You can find more articles by Michael at
Dr. Michael Infantino is a physical therapist. He works with active military members in the DMV region. You can find more articles by Michael at